Downloaded 702 times
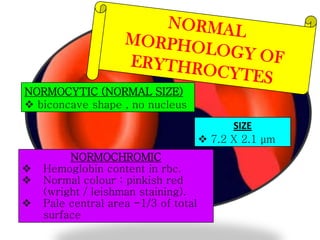
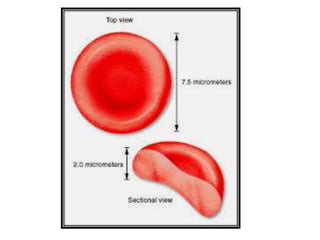
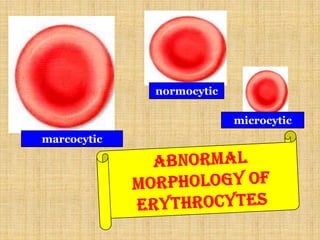
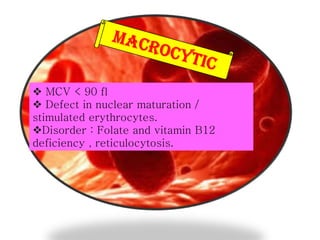
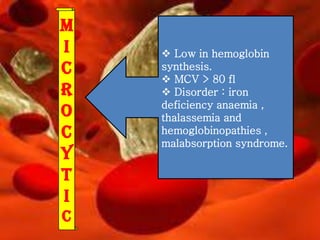
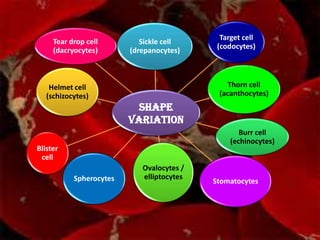
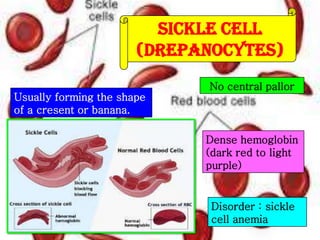
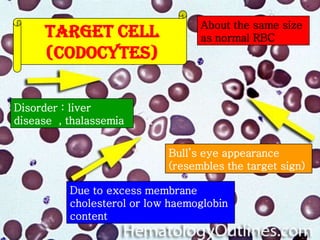
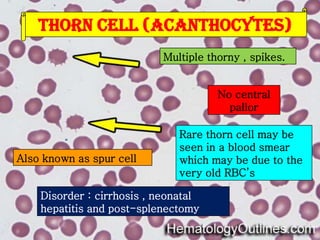
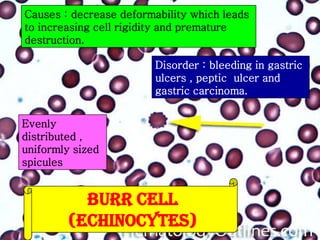
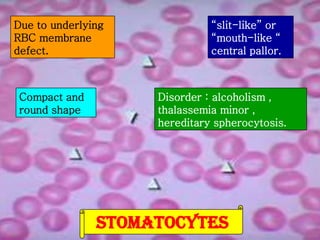
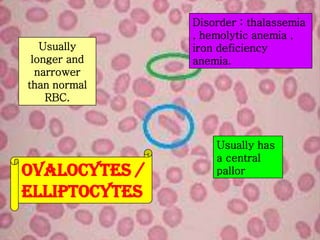
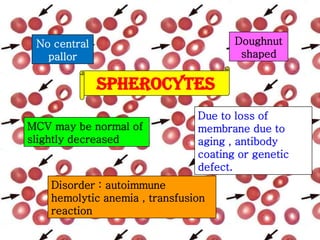
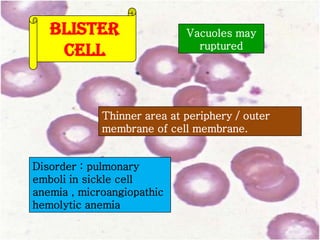
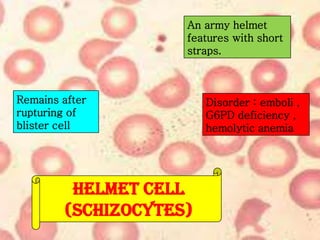
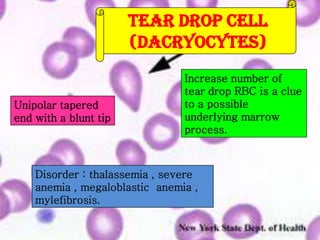
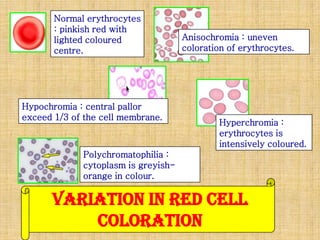
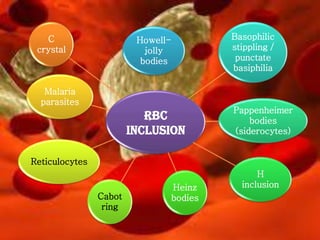
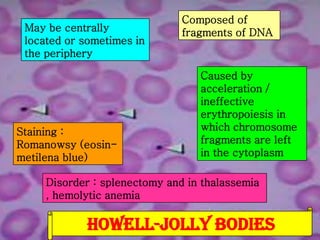
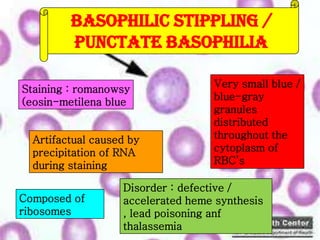
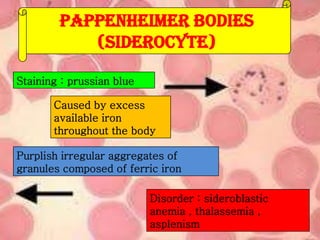
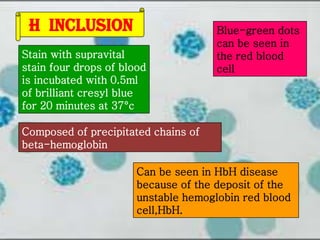
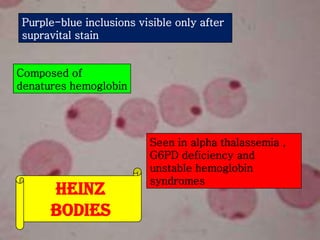
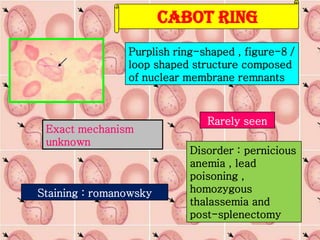
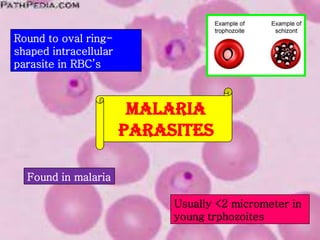
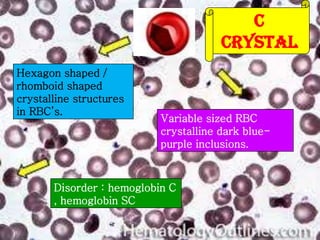


This document provides information on various types of red blood cell morphologies seen on blood smears, including normal and abnormal shapes and inclusions. It describes normocytic and normochromic red blood cells as well as variations such as microcytic, macrocytic, poikilocytes (variations in shape), anisocytosis (variation in size), and polychromasia (variation in color). Specific abnormal red blood cells and inclusions are defined such as sickle cells, target cells, Howell-Jolly bodies, basophilic stippling, malaria parasites, and reticulocytes. Causes and disorders are provided for each abnormal finding.