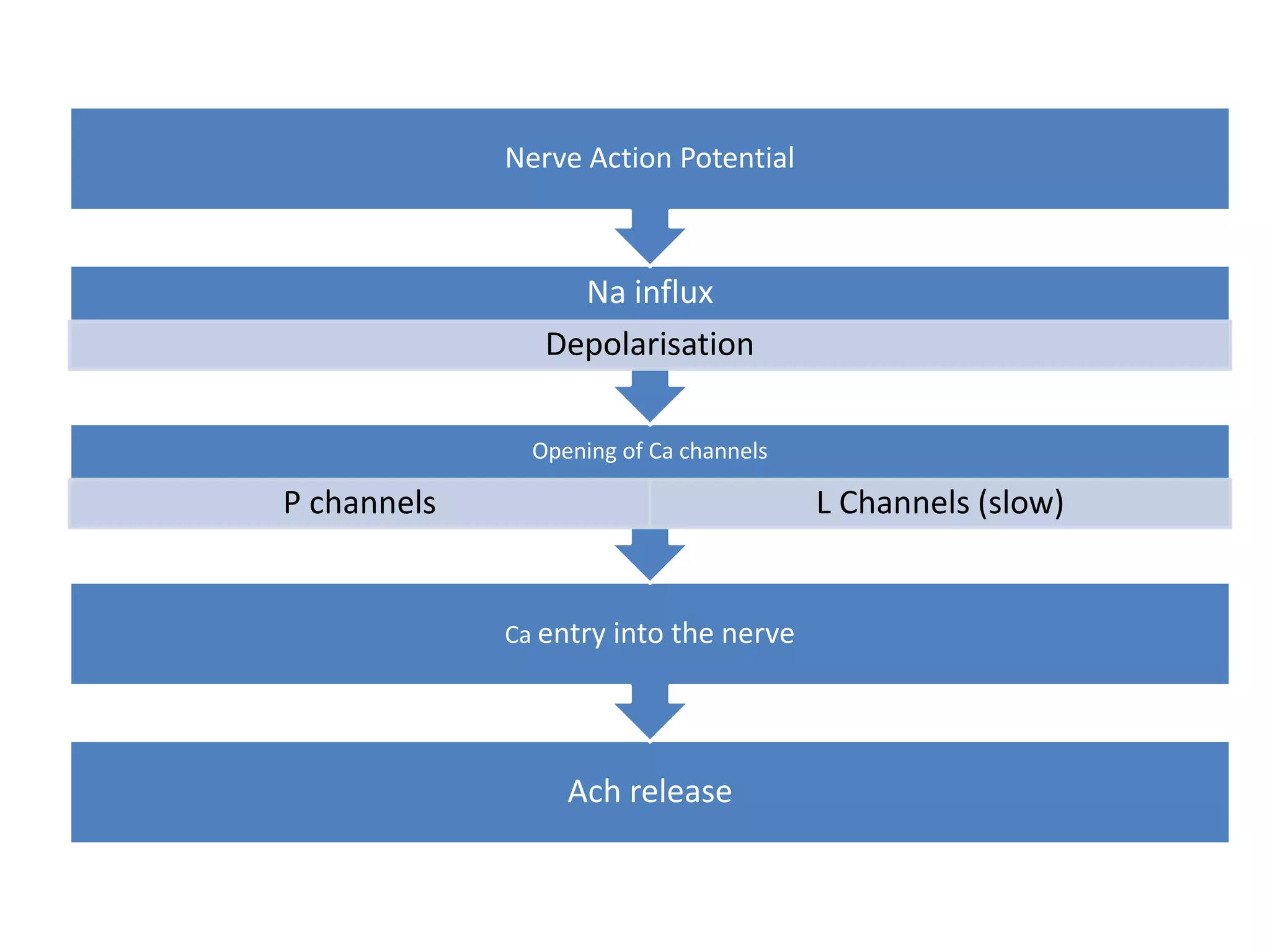
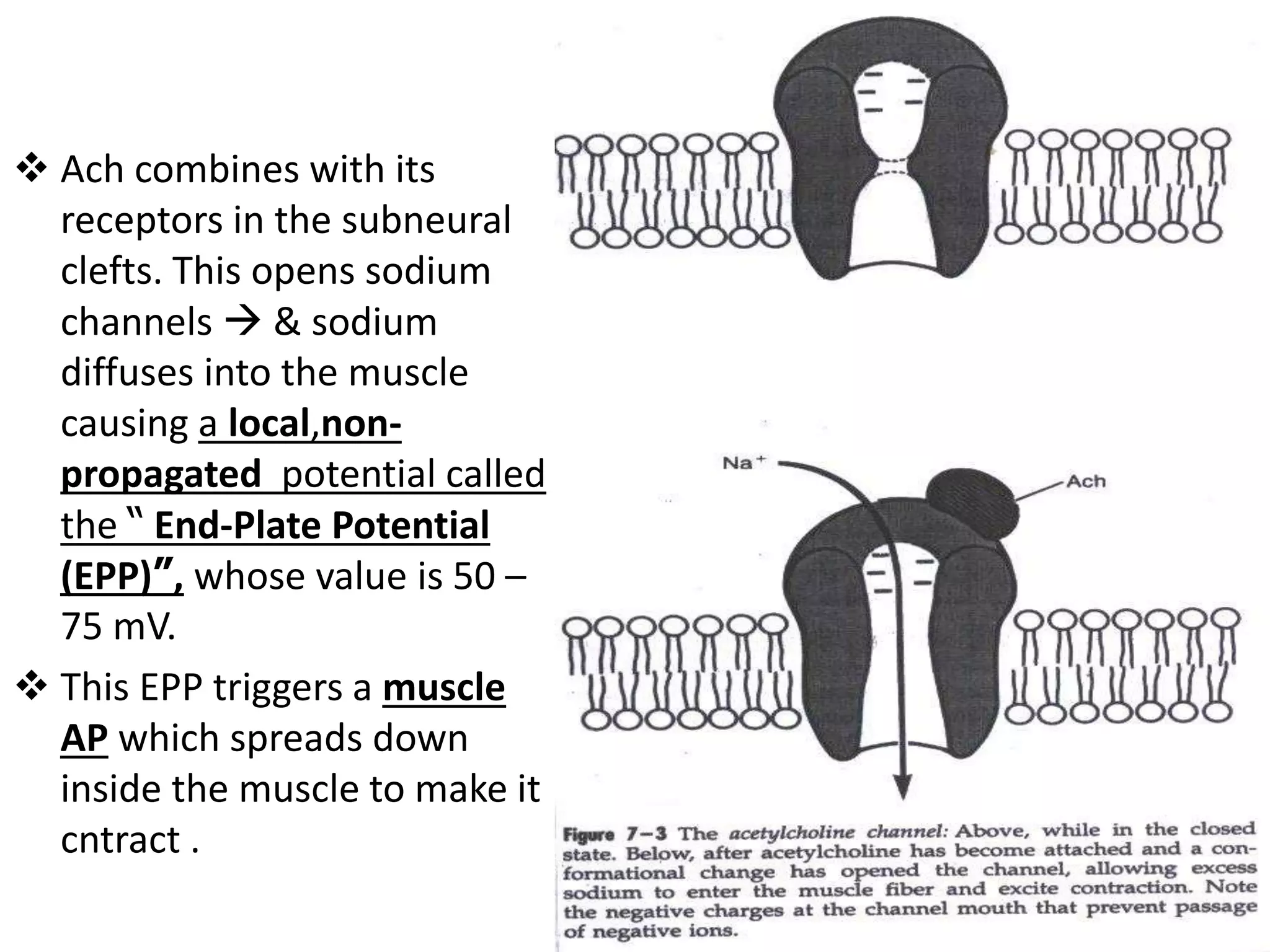
The neuromuscular junction consists of the motor neuron axon terminal, synaptic cleft, and motor end plate of muscle fiber. Acetylcholine is synthesized in the neuron, stored in vesicles, and released into the synaptic cleft upon arrival of an action potential. It binds nicotinic receptors on the muscle, opening ion channels and initiating an endplate potential that spreads and causes muscle contraction. Acetylcholine is then broken down by acetylcholinesterase to terminate its effect. Nondepolarizing muscle relaxants block transmission by preventing acetylcholine binding, while depolarizing relaxants directly activate ion channels. Anesthetic drugs can also impact transmission through desensitization or channel blockade effects.