Downloaded 34 times
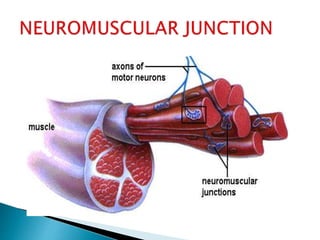
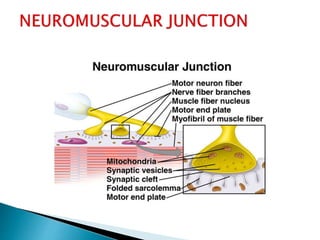
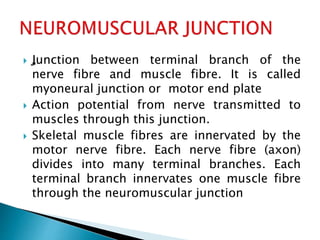
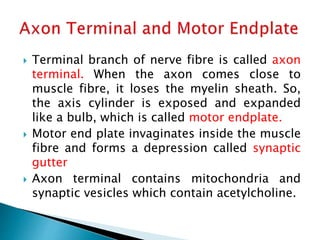
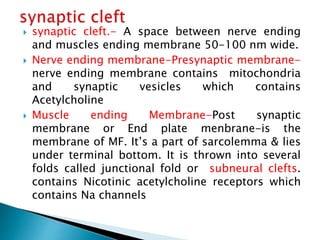
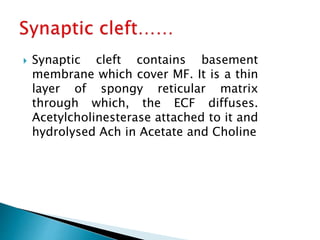
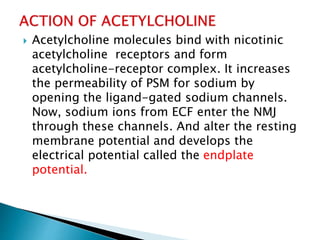
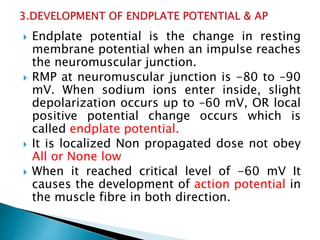

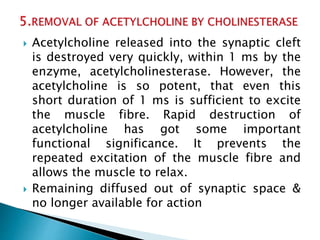
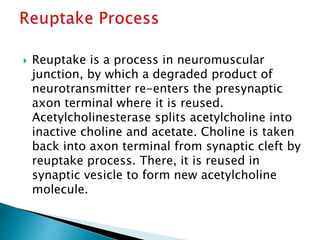

The neuromuscular junction is where the terminal branch of a nerve fiber meets with a muscle fiber. An action potential is transmitted from the nerve to the muscle through this junction, allowing for muscle contraction. The nerve fiber terminal contains acetylcholine vesicles which release acetylcholine into the synaptic cleft when an action potential arrives. Acetylcholine then binds to nicotinic receptors on the muscle fiber, opening sodium channels and generating an endplate potential that can trigger a muscle action potential if it surpasses a threshold. Acetylcholine is quickly broken down by acetylcholinesterase to allow muscle relaxation.





















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













