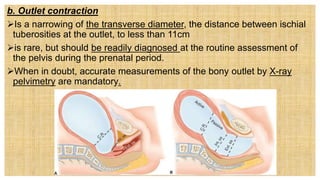
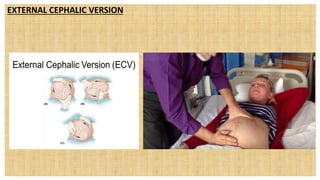
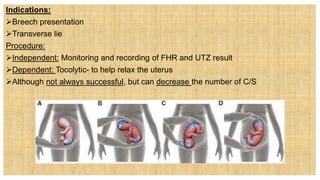
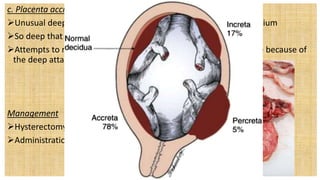
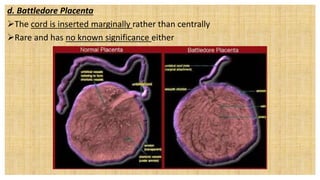
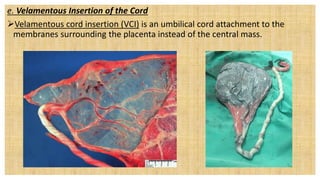
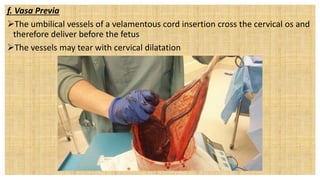
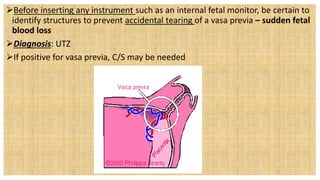
This document discusses various complications that can occur with the passage of the baby during birth due to issues with the mother's pelvis or birth canal. It describes how narrowing or contractions of the inlet, midpelvis, or outlet can cause cephalopelvic disproportion. It also discusses other potential issues like anomalies of the placenta such as placenta succenturiata which could lead to hemorrhage if lobes are retained, and vasa previa which involves blood vessels crossing the cervix and can cause bleeding with dilation. External cephalic version and trial of labor are mentioned as potential approaches to addressing some of these complications.