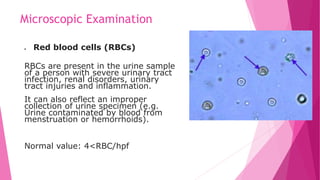
The document discusses various diagnostic tests involving specimen collection and testing, including proper procedures for collecting stool, urine, and other specimens. It covers the nursing responsibilities associated with specimen collection, as well as explanations of various urine tests including urinalysis, urine dipstick testing, and microscopic urine examination. The goal of specimen collection and testing is to provide important information for diagnosing health problems and monitoring treatment responses.




































































![References:
Audrey Berman . . . [et al.]. – 9th ed. (2012) KOZIER &
ERB’S Fundamentals of NURSING Concepts, Process, and
Practice.
NursesLabs. Date Retrieved: March 2018](https://image.slidesharecdn.com/03laboratorytestspart2-210313154329/85/laboratory-tests-part-2-71-320.jpg)























































































