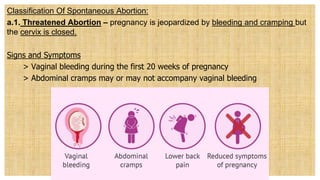
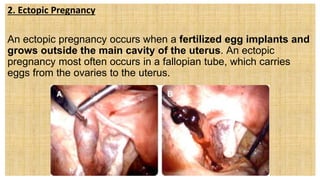
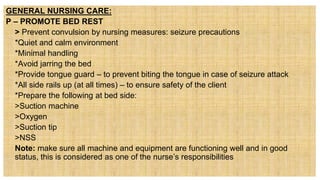
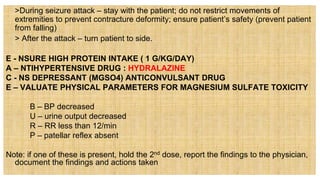
The document discusses the nursing care plan for mothers experiencing pregnancy complications, outlining assessment, diagnosis, planning, implementation, and evaluation stages. It covers various types of pregnancy complications, including spontaneous abortion, septic abortion, and ectopic pregnancy, detailing symptoms, management, and potential outcomes. The importance of maternal and fetal welfare, psychological health, and the necessity of monitoring and treatment interventions are emphasized throughout.