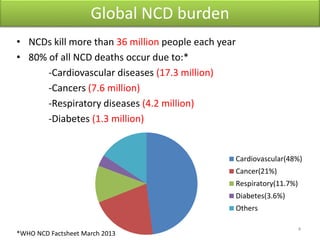
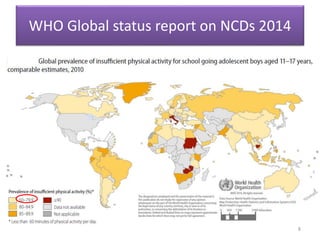
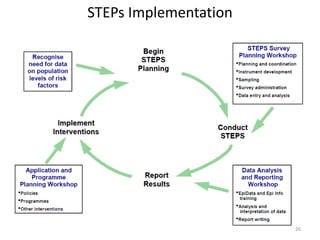
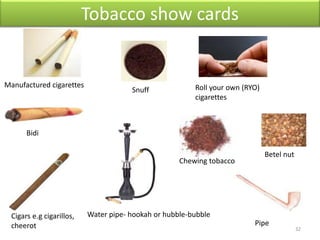
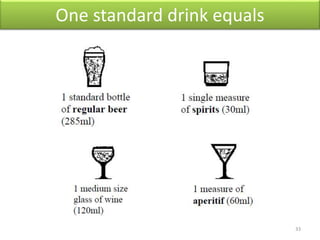
This document discusses NCD risk factor assessment and surveillance. It outlines the global burden of NCDs, risk factors, and the WHO STEPs approach for NCD risk factor surveillance. The STEPs approach involves standardized collection of risk factor data through questionnaires, physical measurements, and blood samples. Challenges with NCD surveillance in India include obtaining accurate anthropometric and behavioral data due to low awareness, cultural and language diversity, field conditions, and tracking subjects over time. Consistent surveillance is important for monitoring trends, evaluating interventions, and planning prevention programs to reduce the NCD burden through modifiable risk factors.