Downloaded 88 times







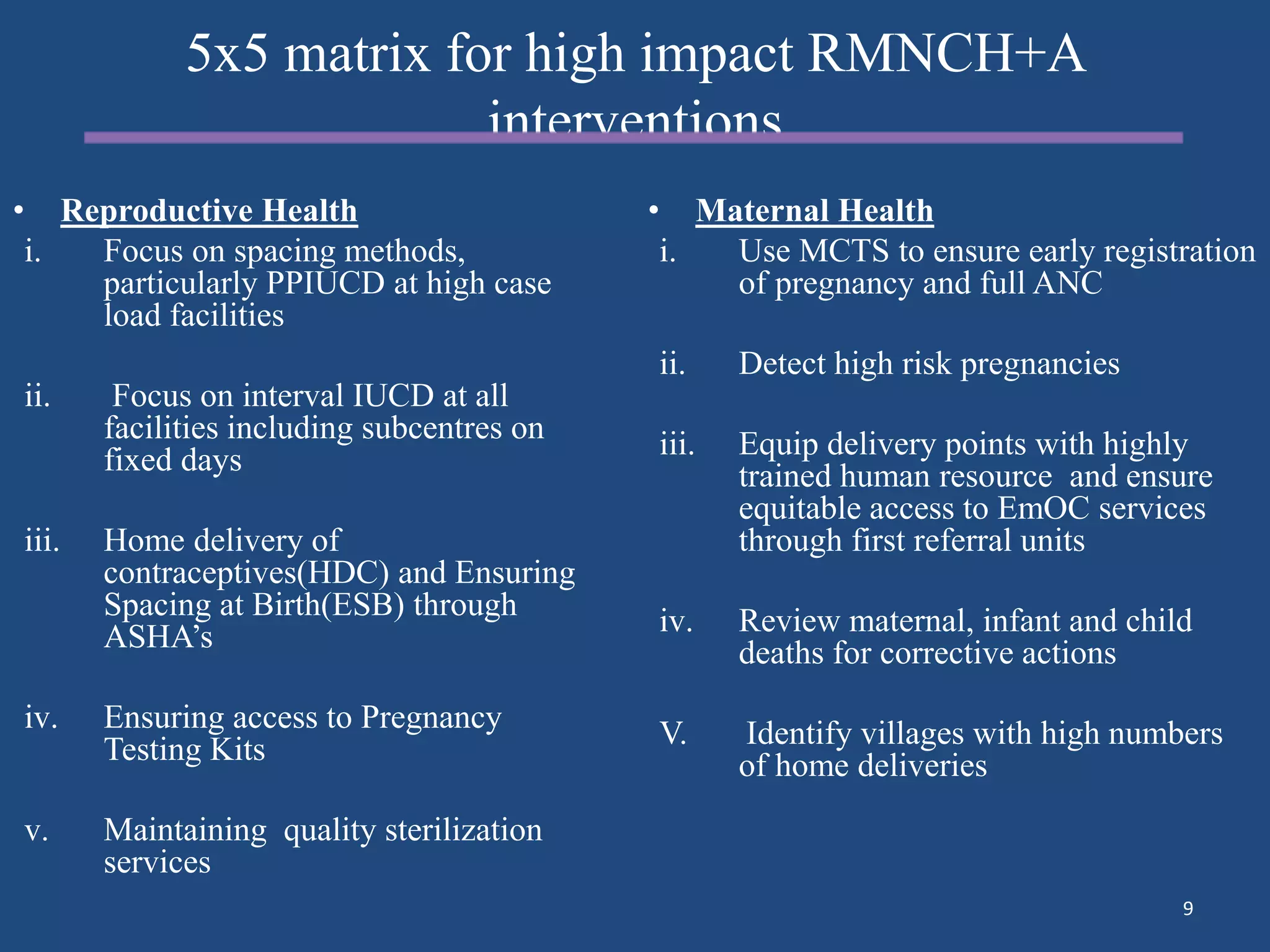

































The document discusses India's RMNCH+A (Reproductive, Maternal, Newborn, Child Health Plus Adolescent) approach, which aims to provide integrated health services across different life stages through a continuum of care. Key aspects of the approach include reducing mortality and malnutrition, increasing immunization coverage, and strengthening service delivery through community health workers. Progress is monitored using indicators tracked in scorecards that measure coverage of important interventions like antenatal care, institutional deliveries, postnatal checks, and child nutrition. The approach emphasizes addressing the needs of vulnerable groups like adolescent mothers through new initiatives for maternal and newborn care, child health, family planning and adolescent health.



































































