Downloaded 53 times

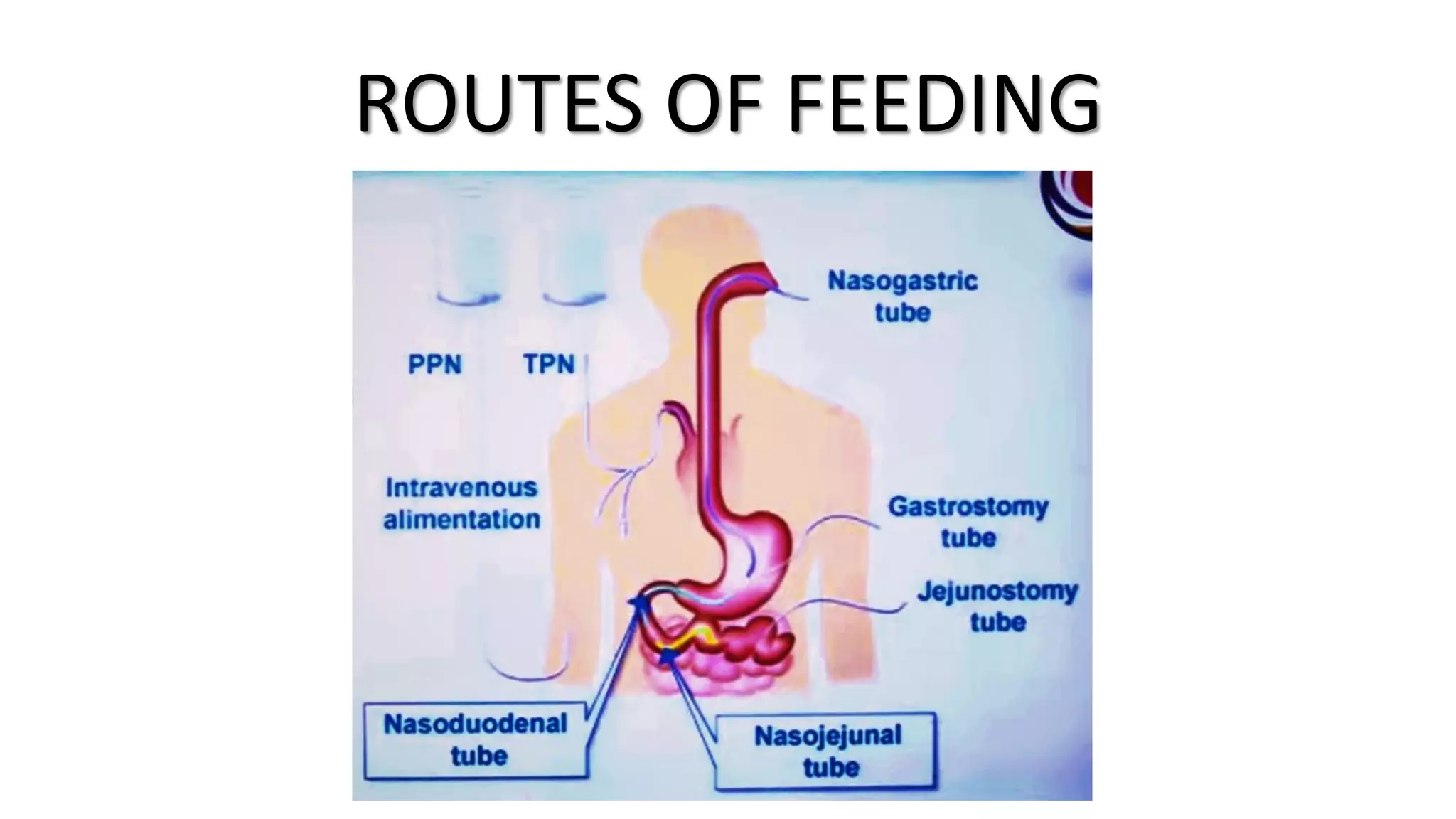








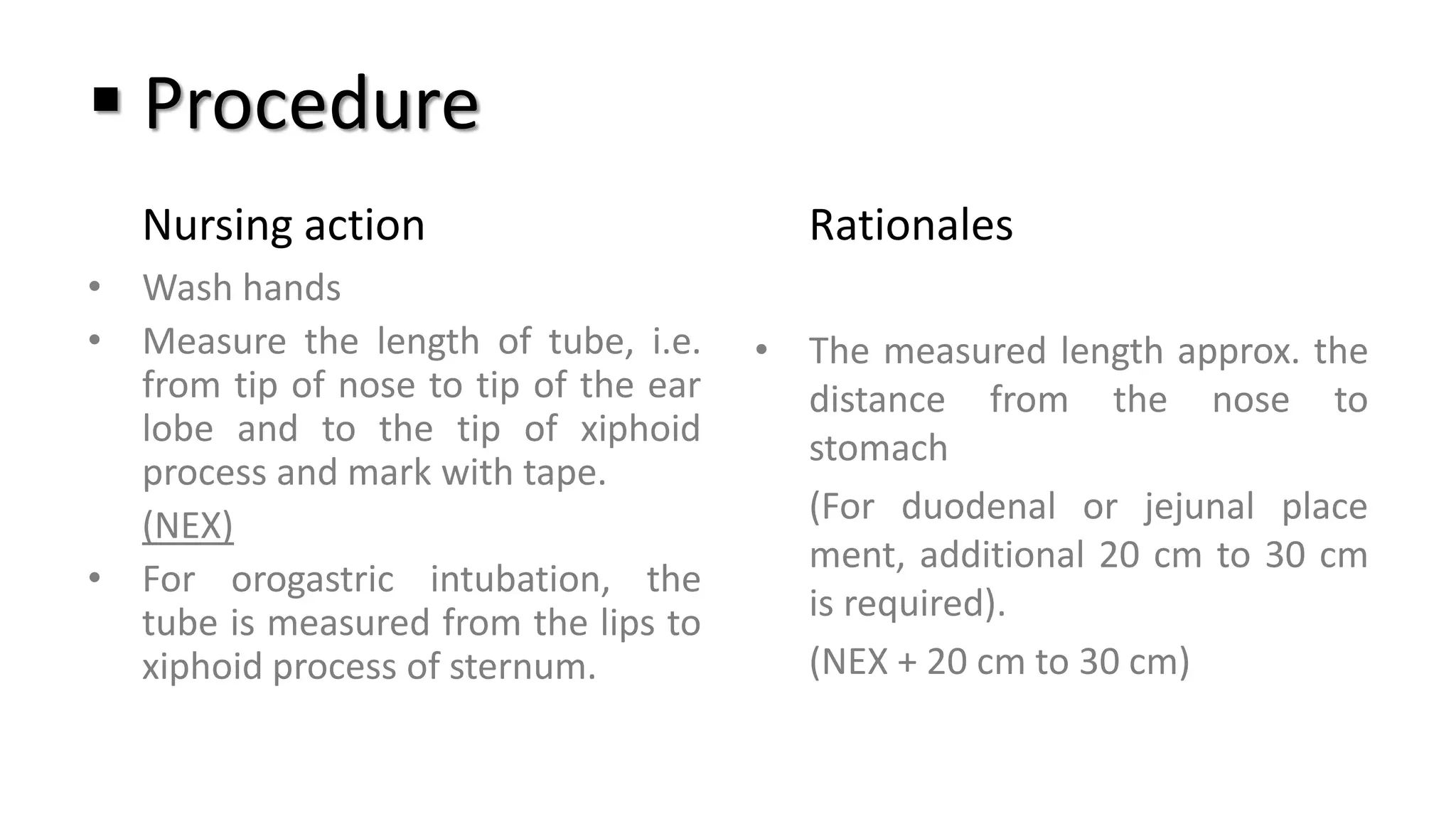
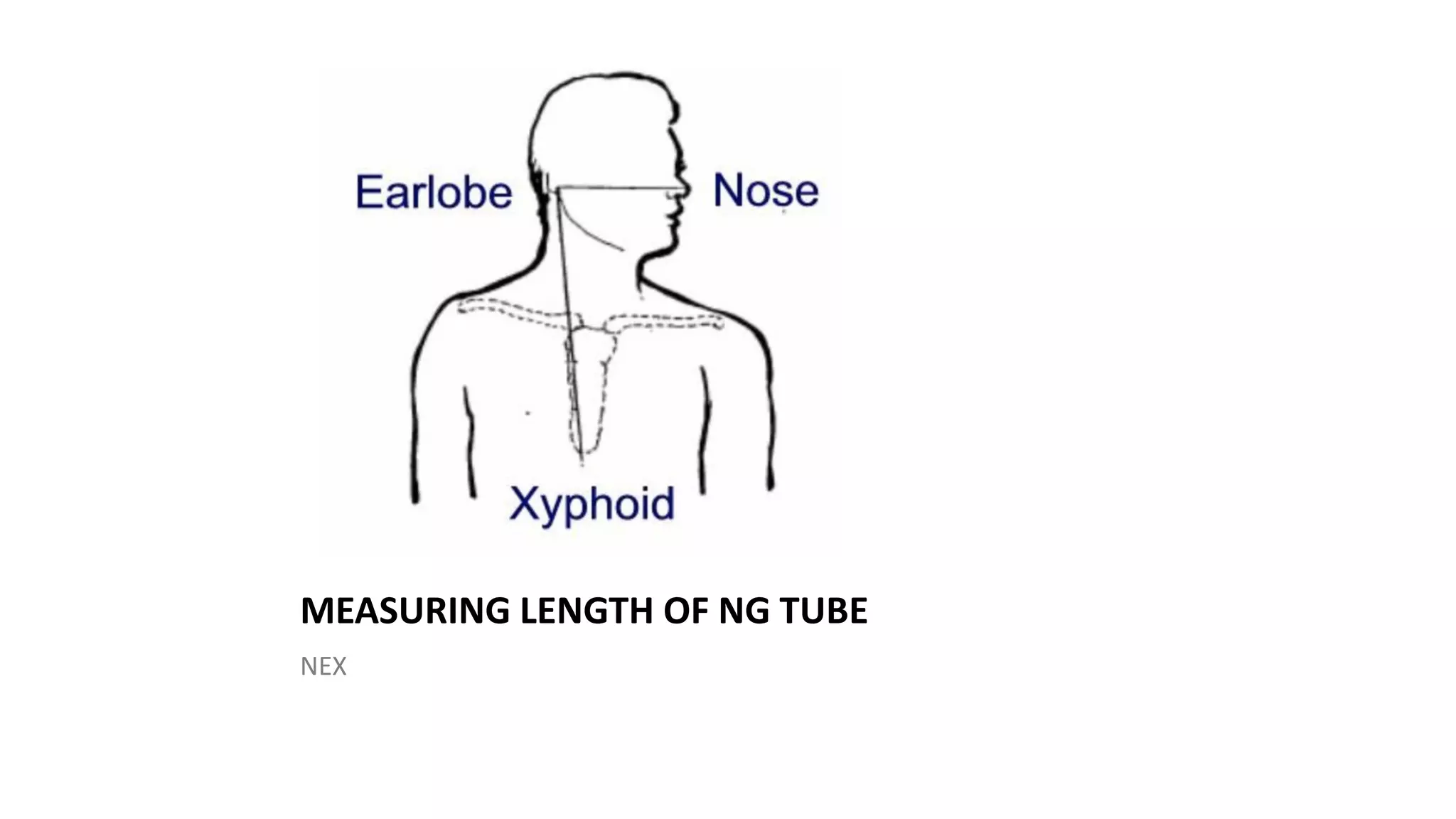























The document discusses the nasogastric tube insertion procedure and feeding. It describes inserting a tube through the nose and into the stomach to administer feeding or remove gastric contents. Key steps include measuring the tube length, lubricating and inserting it while having the patient swallow, then checking the placement. Feeding is then given by filling a syringe with formula and allowing it to flow through the tube into the stomach by gravity in small amounts. Residual contents are checked before and after feeding.









































































