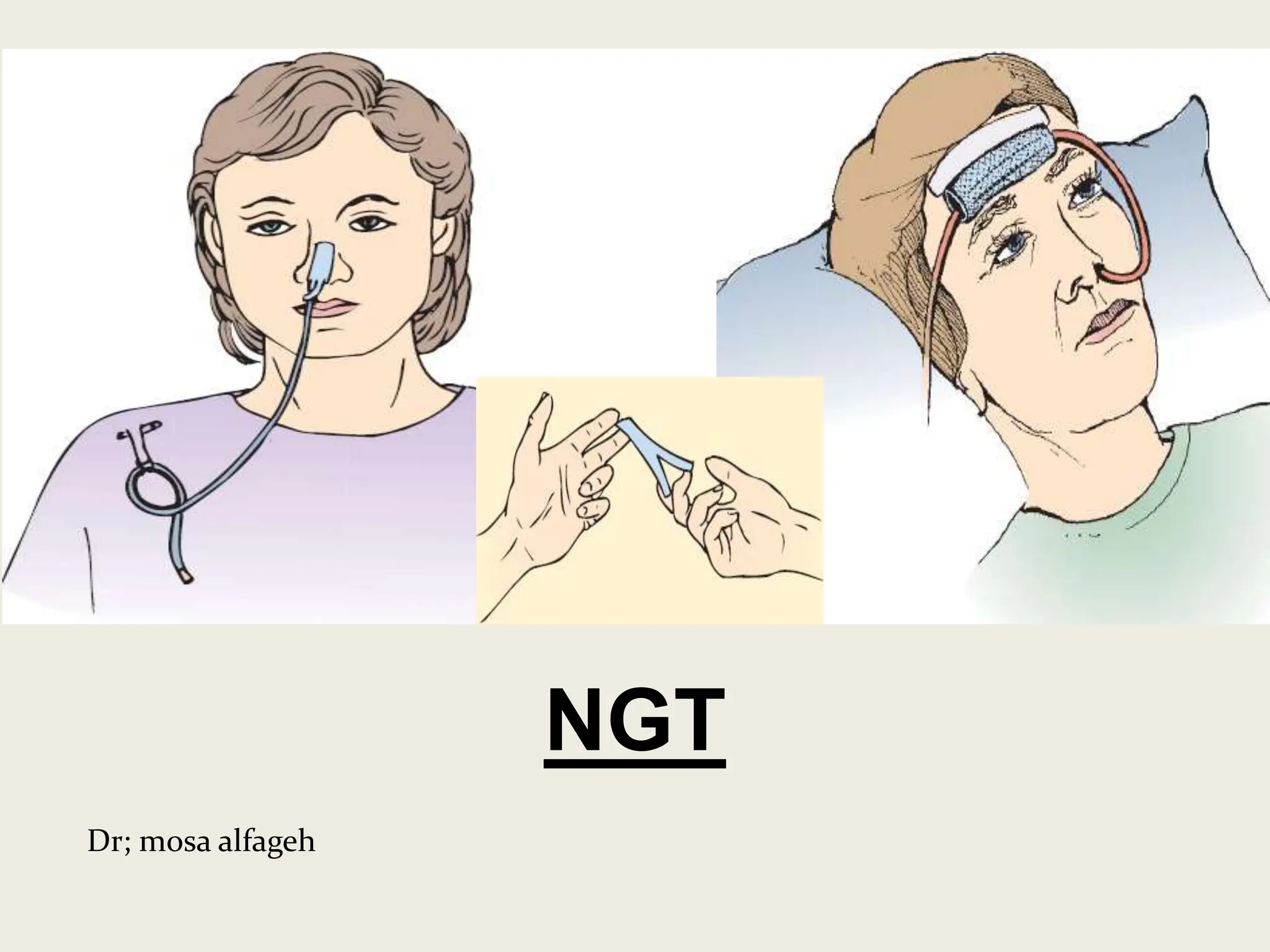
This document provides information about nasogastric tube (NGT) insertion and feeding. It defines NGT as the passage of a tube through the nose or mouth into the stomach. The purposes of NGT insertion include feeding patients who cannot eat orally, diluting/removing poisons, controlling gastric bleeding, and relieving vomiting/distension. Indications for NGT include inability to eat orally due to various medical conditions. The document outlines the procedure for NGT insertion and feeding, including necessary supplies, patient preparation, confirming tube placement, and post-care. It also defines gastric gavage and describes gastrostomy and jejunostomy feeding methods.