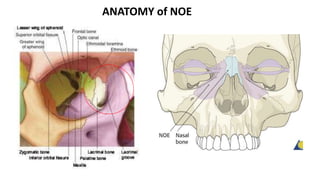
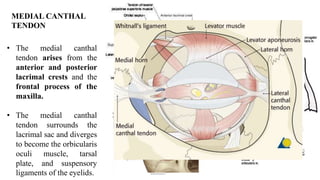
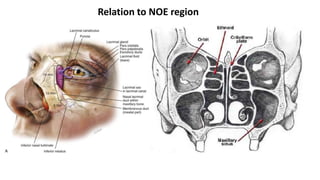
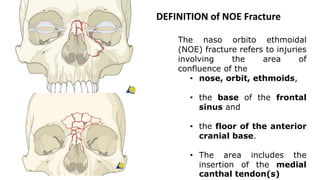
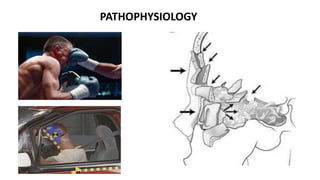
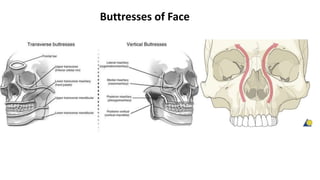
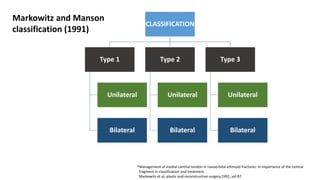
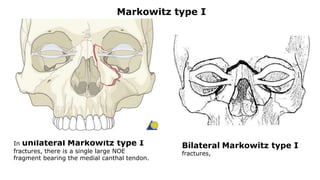

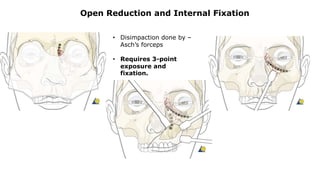
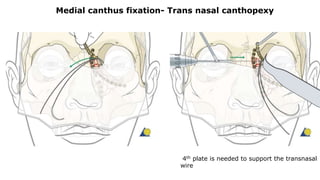
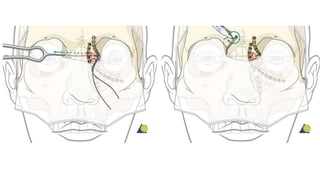
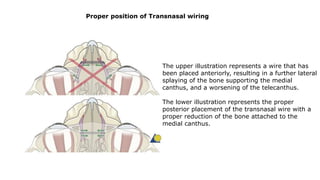
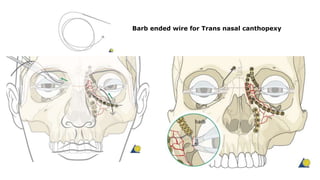
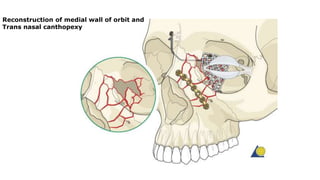
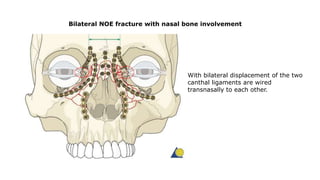


1) NOE fractures involve the nose, orbit, ethmoids, and frontal sinus floor, including the medial canthal tendon attachment area. 2) Classification systems include the Markowitz system of Types I-III based on medial canthal tendon involvement and displacement. 3) Treatment involves open reduction and internal fixation to restore anatomy, including medial canthal tendon reconstruction using transnasal wiring or plating.











































































