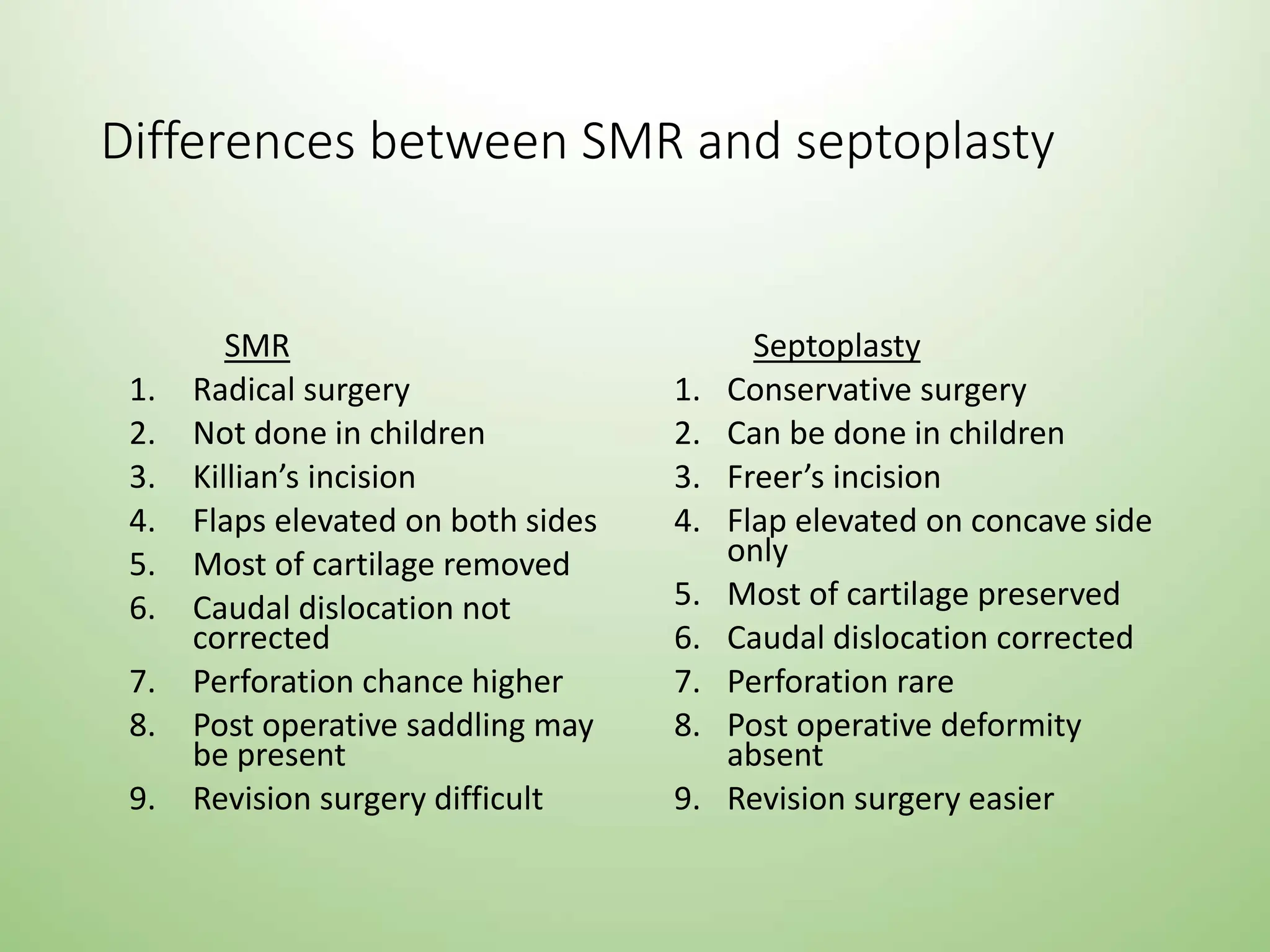
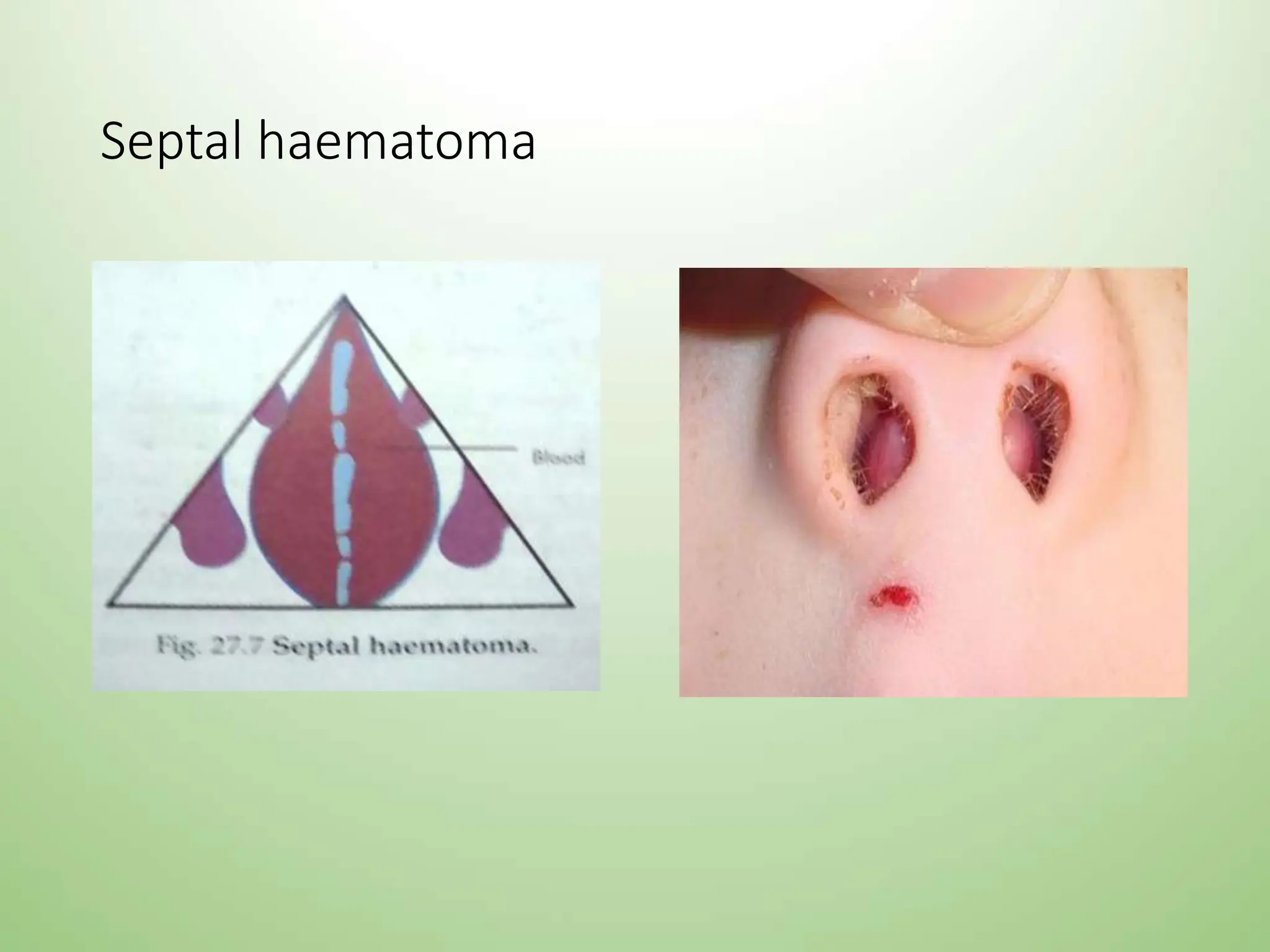
The document discusses the anatomy, conditions, and surgical treatments related to the nasal septum, detailing its structure and the impact of injuries and diseases. It covers various types of septal fractures, deviations, and complications such as septal hematoma and perforation, outlining their clinical features and treatment approaches. Surgical interventions like submucosal resection (SMR) and septoplasty are described, highlighting their indications, contraindications, procedures, and potential post-operative complications.