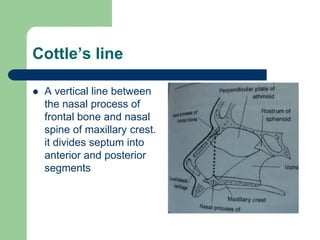
The nasal septum is made up of three parts and provides structural support to the nose. Deviations, injuries, or infections of the nasal septum can cause problems like nasal obstruction or recurrent nosebleeds. Surgical procedures like submucous resection (SMR) and septoplasty are commonly used to correct deviated septums. Complications of these surgeries or injuries to the septum can include hematomas, abscesses, or perforations of the nasal septum if not properly treated.