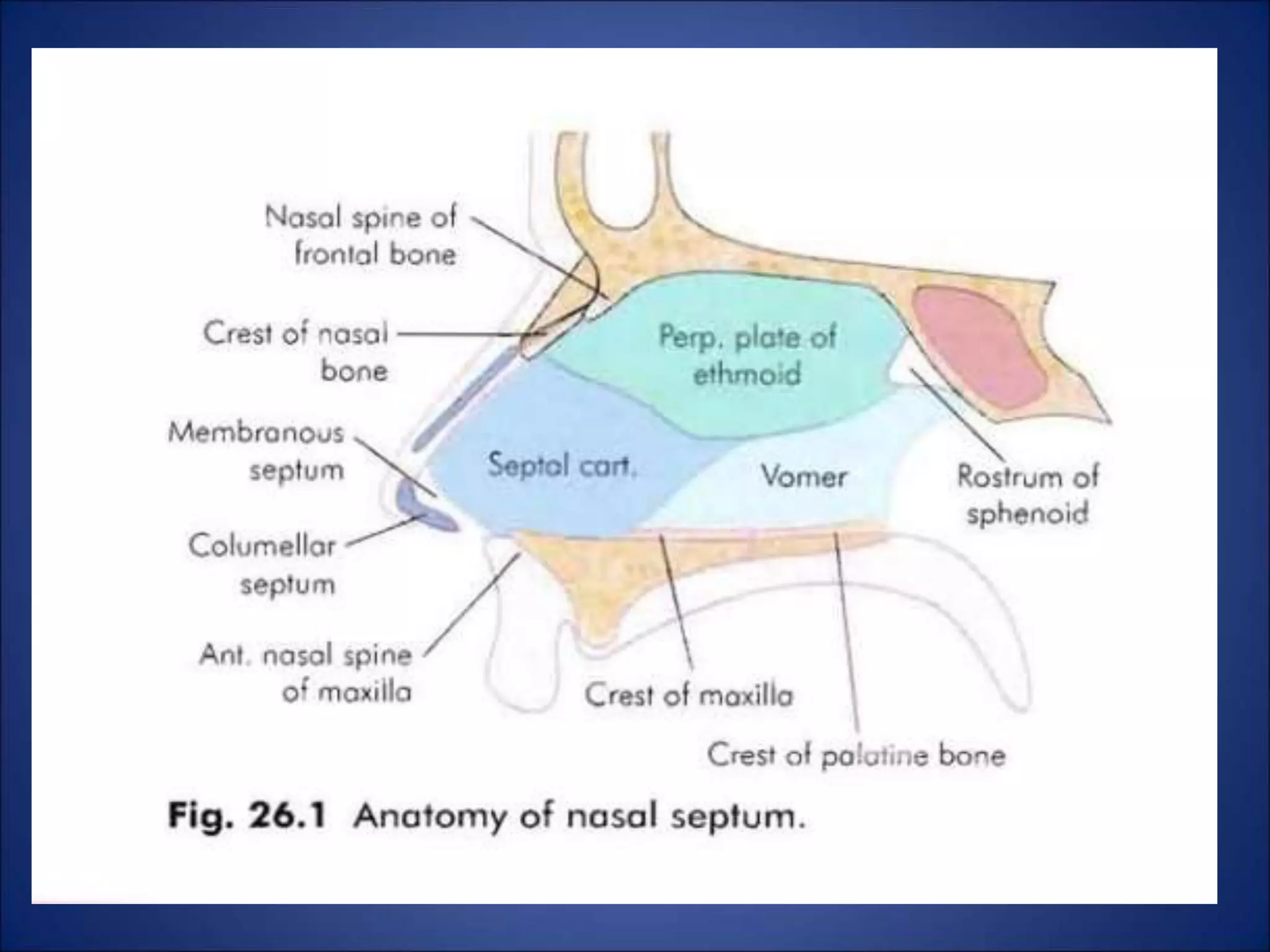
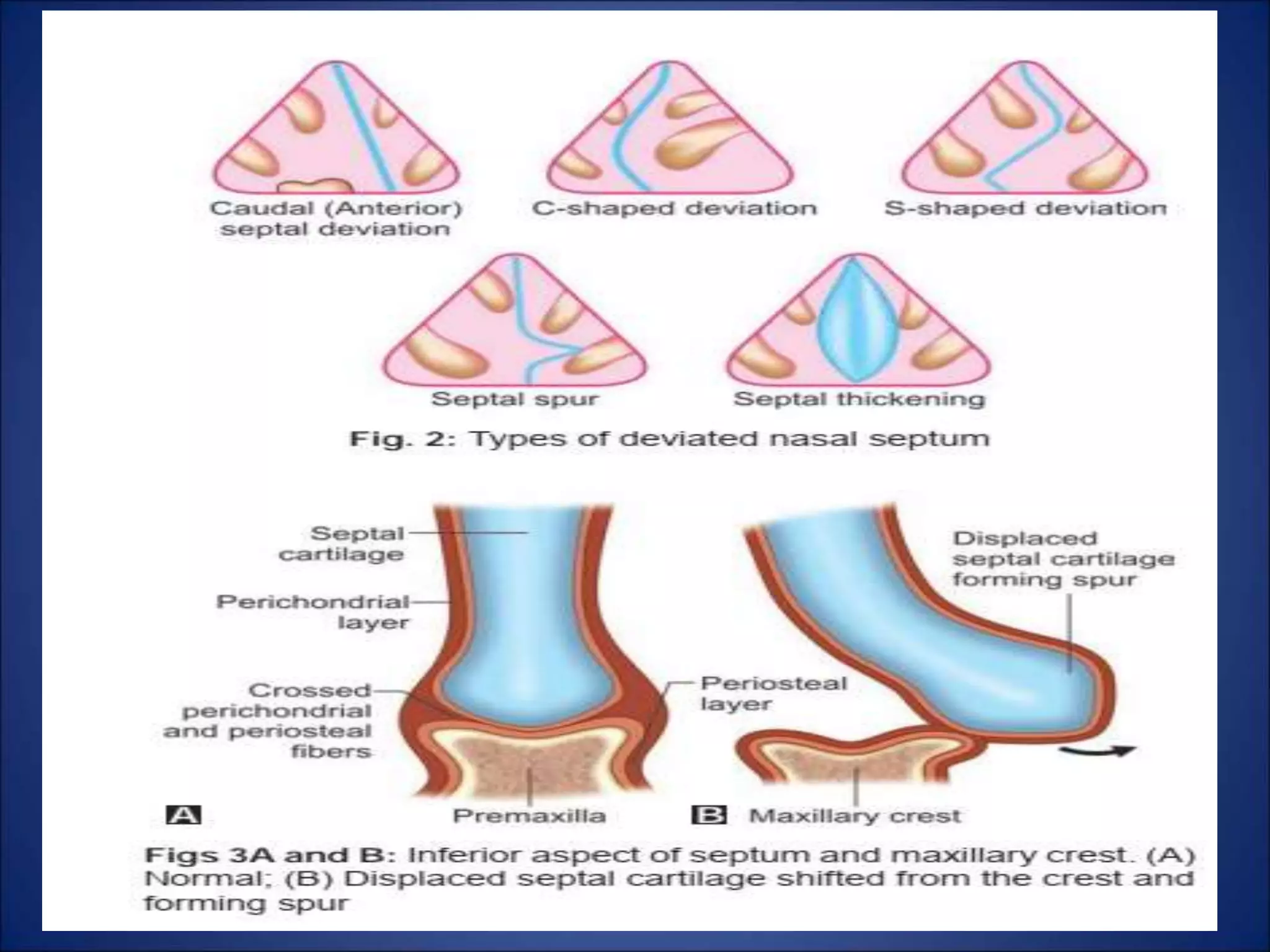
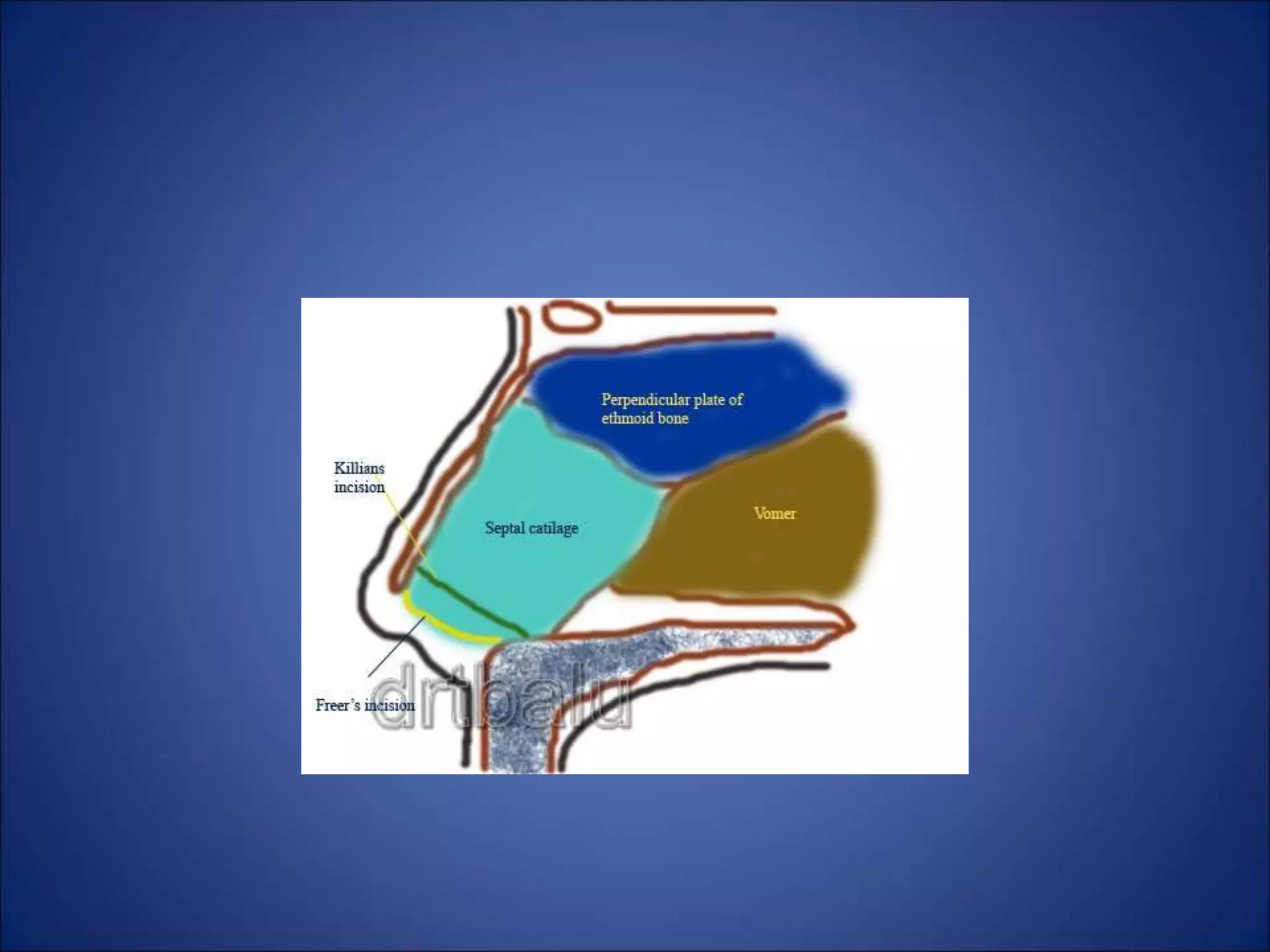
This document discusses deviated nasal septum, including causes, types, symptoms, signs, and surgical treatments. Common causes of septal deviation include direct trauma, birth molding, and differential growth between the septum and palate. Deviations can involve cartilage and/or bone, and be classified as spurs, C-shapes, S-shapes, or dislocations. Symptoms are usually nasal obstruction. Surgical treatments include submucous resection (SMR) and septoplasty. SMR involves removing deviated tissue, while septoplasty is more conservative, mobilizing and straightening the septum without full resection. Both aim to improve nasal breathing.


















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












