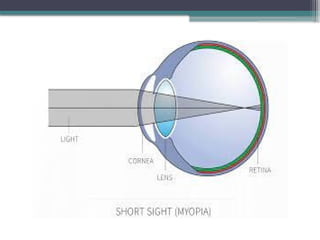
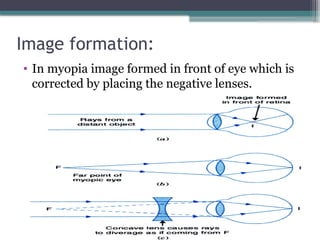
The document discusses myopia, a refractive error characterized by focused light in front of the retina, and explores its optics, classifications, and management strategies. It details various types of myopia, risk factors including genetics and lifestyle, and symptoms associated with both simple and pathological forms. Additionally, it covers the complications related to myopia and types based on severity.