Mumps & Rubella.pptx
•Download as PPTX, PDF•
0 likes•48 views

This document summarizes information about Mumps and Rubella. Mumps is caused by the mumps virus, an RNA paramyxovirus. It causes swelling of the parotid glands. The virus is transmitted through respiratory droplets. Complications can include orchitis. Vaccination with the MMR vaccine provides protection. Rubella, also known as German measles, is caused by the rubella virus, an RNA togavirus. It causes a rash and lymphadenopathy. Congenital rubella syndrome can occur if a pregnant woman is infected, causing birth defects. The rubella vaccine is a live attenuated vaccine that provides lifelong immunity in 95% of cases. Global vaccination strategies

More Related Content
Similar to Mumps & Rubella.pptx
Similar to Mumps & Rubella.pptx (20)
More from Rahul Netragaonkar
More from Rahul Netragaonkar (20)
Recently uploaded
Recently uploaded (20)
Mumps & Rubella.pptx
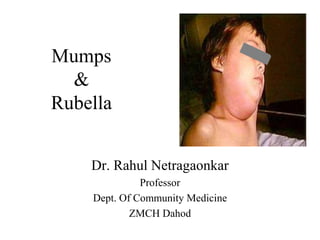
- 1. Mumps & Rubella Dr. Rahul Netragaonkar Professor Dept. Of Community Medicine ZMCH Dahod
- 2. • Mumbling Speech - Mumps : • Name "mumps" comes from "lump" or "mumble."
- 3. Mumps • Acute viral illness • Parotitis and orchitis described by Hippocrates in 5th century BC • Viral etiology described by Johnson and Goodpasture in 1934 • Frequent cause of outbreaks among military personnel in pre vaccine era
- 4. MUMPS • Acute infectious disease due to “myxovirus parotiditis” ; RNA paramyxovirus (Genus Rubulavirus) affecting mainly glands and nervous system • Clinically the disease is recognized by enlargement of one or both parotid glands with tenderness. • Worldwide distribution. • Morbidity is high. Mortality is less.
- 5. Mumps Epidemiology • Reservoir Human Asymptomatic infections may transmit • Transmission Respiratory drop nuclei • Temporal pattern Peak in late winter and spring • Communicability Three days before to four days after onset of active disease
- 6. MUMPS • AGENT FACTORS: • A)Agent: Myxovirus parotiditis is a RNA virus of the myxovirus family. The virus can be grown in chick embryo or tissue culture. There is only one serotype.
- 7. Mumps Virus • Paramyxovirus • RNA virus • One antigenic type • Rapidly inactivated by chemical agents, heat, and ultraviolet light
- 8. MUMPS • The virus can be • A)Isolated from the saliva or from swabs taken from the surface of STENSON’S DUCT. • Virus has also been found in the blood, urine, human milk, and in the CSF. • A) PERIOD OF COMMUNICABILITY: • Usually 4-6 days before the onset of symptoms and a week thereafter. The period of maximum infectivity is just before and at the onset of parotitis.
- 9. • SOURCE OF INFECTION: Both clinical and sub clinical cases. • Sub clinical cases accounts for 30-40% of all cases.
- 10. MUMPS • A) SECONDARY ATTACK RATE: • Estimated to be about 86%
- 11. HOST FACTORS • a)AGE AND SEX: Mumps is the most frequent cause of parotitis in children in the age group of 5-15 years. The average age of incidence of mumps is higher than with measles, chicken pox or whooping cough.
- 12. MUMPS • MODE OF TRANSMISSION:The disease is spread mainly by droplet infection and after direct contact with an infected person. • INCUBATION PERIOD; Varies from 2-3 weeks usually 18 days. • CLINICAL FEATURES:30-40% of cases are sub clinical characterized by pain and swelling in either one or both parotid glands and involves the sublingual submandibular glands.
- 13. Mumps Pathogenesis • Respiratory transmission of virus • Replication in nasopharynx and regional lymph nodes • Viremia 12-25 days after exposure with spread to tissues • Multiple tissues infected during viremia
- 14. Mumps Clinical Features • Incubation period 14- 18 days • Nonspecific prodromal phase of myalgia, malaise, headache, low-grade fever • Parotitis in 30%-40% • Up to 20% of infections asymptomatic
- 15. Mumps Clinical Case Definition • Acute onset of unilateral or bilateral tender, self-limiting swelling of the parotid or other salivary gland lasting more than 2 days without other apparent cause
- 16. MUMPS The disease tends to be more severe in adults than in children. IMMUNITY: One attack clinical or sub clinical will induce life long immunity. ost infants < 6 months of age are immune because of maternal antibodies. • ENVIRONMENTAL FACTORS: • Mumps is largely an endemic disease. Cases occur throughout the year – but peak incidence in wintertime of the year – but peak incidence in winter and spring. Over crowding linked to epidemics
- 17. 17 Complications of Mumps Frequent but not serious: • Orchitis (25-40%): 7-10 days after parotitis,with high fever (Unilateral in 75% orchitis cases, Most common extra-salivary gland manifestation in adults) • Epididymitis • Pancreatitis (4%) • Mild form of meningitis • Thyroiditis, Neuritis, Hepatitis,Ovaritis, • Oophoritis (5% adult women) • Spontaneous abortion(25% in pregnancy) Rare: Hearing loss, Polyarthritis, Encephalitis, Cerebellar ataxia
- 18. • Mumps infection in post-pubertal males can result in swelling of the testicles in 22-30% of affected individuals. • Such swelling may then lead to marked atrophy (shrinkage) of the testicle with poor sperm production as the result.
- 19. Mumps Laboratory Diagnosis • Isolation of mumps virus • Detection of mumps antigen by PCR • Serologic testing – positive IgM antibody – significant increase in IgG antibody between acute and convalescent specimens
- 20. MUMPS • PREVENTION: VACCINE: • Recommended for children over one year of age. • Its use may be considered in susceptible adults, especially males. • Mumps vaccine should not be administered to pregnant women, who are severely ill or who are on Immuno suppressive therapy
- 21. Mumps Vaccine • Composition Live virus (Jeryl Lynn strain) • Efficacy 80% (1 dose) • Duration of Immunity Lifelong • Schedule At least 1 Dose should be administered with measles and rubella as MMR or with measles, rubella and Varicella as MMRV
- 22. Mumps (MMR) Vaccine Indications • One dose (as MMR) for preschool-age children 12 months of age and older and persons born during or after 1957 not at high risk of mumps exposure • Second dose (as MMR) for school-age children and adults at high risk of mumps exposure (i.e., healthcare personnel, international travelers and students at post-high school educational institutions
- 23. MMR Adverse Reactions • Fever 5%-15% • Rash 5% • Joint symptoms 25% • Thrombocytopenia <1/30,000 doses • Parotitis* rare • Deafness* rare • Encephalopathy <1/1,000,000 doses *reactions usually attributed to the mumps component
- 24. MMR Vaccine Contraindications and Precautions • Severe allergic reaction to vaccine component or following a prior dose • Pregnancy • Immunosuppression • Moderate or severe acute illness • Recent blood product
- 25. Vaccine Storage and Handling MMR Vaccine • Store 35o - 46o F (2o - 8o C) (may be stored in the freezer) • Store diluent at room temperature or refrigerate • Protect vaccine from light • Discard if not used within 8 hours reconstitution
- 26. MIG • a) IMMUNO GLOBULIN: • A specific Immuno globulin (MIG) is available. • CONTROL: The control of mumps is difficult because the disease is infectious before a diagnosis can be made. Due to long I.P, sub clinical cases, - it is difficult to control mumps. • Isolation of cases. • Disinfection of the articles. • Contacts kept under surveillance
- 27. RUBELLA (GERMAN MEASELS • RUBELLA or German Measles is an acute child hood infection usually mild of short duration (3 days) and accompanied by low- grade fever, lymphadenopathy and a maculopapular rash. Infection in early pregnancy may result in serious congenital defects like PDA, cataract and deafness. Rubella in pregnancy can also cause spontaneous abortion and stillbirth.
- 28. RUBELLA HISTORY • HISTORY: • 1941 – Norman Gregg – reported rubella infection in pregnancy WHICH IN TURN linked to congenital anomalies including congenital cataracts. • 1962 – The virus was isolated. • 1967 – Live attenuated vaccine was developed.
- 29. Epidemiological Determinants AGENT: • It is a RNA virus of the Toga virus family. • Virus can be recovered from the cases of Rubella, from naso- pharynx, throat, blood, CSF and urine. • It can be propagated in cell culture.
- 30. SOURCE OF INFECTION • Clinical or sub clinical cases of rubella. Most of the infections are sub clinical. Infants born with infection may shed the virus, for many months. Vaccine virus is not communicable.
- 31. AGENT&HOST FACTORS: • Period of Communicability • Less communicable than measles. • Probably one week prior to symptoms to a week after appears.
- 32. HOST FACTORS • a) AGE: Mainly a disease of child hood in age group of 3 – 10 yrs. • - Persons aged > 15. Yrs now account for over 70% of cases in developed countries. This is changing epidemiological pattern with wide coverage of immunization. • IMMUNITY: One attack results life long immunity. 40% women of childbearing age may remain susceptible to rubella
- 33. EPIDEMIOLOGY • ENVIRONMENTALFACTORS: Seasonal variation is present, temperate zones every 4-9 yrs. • TRANSIMISSION: Droplets from nose and throat and droplet nuclei transmit the virus directly from person to person during communicability period. • -The portal of entry is via respiratory route. • - Vertical transmission is also present.
- 34. CLINICALF EATURES • CLINICAL FEATURES: 50-65% of infections are asymptomatic. • a)PRODROMAL: Symptoms like coryza, sore throat, and low-grade fever – herald the onset of viraemia. • b)LYMPHADENOPATHY:Posterior auricular lymph nodes, and posterior cervical group will be enlarged 7 days before rash appearance and it continues 10-14 days after the rash. Some times no lymphadenopathy.
- 35. CLINICALFEATURES • a) RASH: Appears first on face. Rash is like minute, discrete, pinkish, macular rash and not confluent. Rash spreads to trunk and extremities. Rash disappears by 3 rd day. • b) COMPLICATIONS: • - Arthralgia • - Encephalitis (rare) • - Thrombocytopenia purpura • Congenital anomalies of newborn baby
- 36. DIAGNOSIS OF RUBELLA • By virus isolation and serology. 1. - Throat swabs should be cultured for virus isolation. Most widely used test is haemagglutination inhibition test (HAI). • - 4-fold rise in HI antibody titer in paired sera or presence of – IgM in a single serum sample after 2 weeks of rash is diagnostic of rubella. • - More sensitive serological tests include Elisa test and radio immune assay.
- 37. Congenital Rubella Syndrome • Refers to infants born with defects secondary to intrauterine infection or with defects some time after birth. Congenital infection is diagnosed by - Rubella infection inhibits cell division. – reason for congenital malformation and low birth weight.
- 38. CONGENITAL RUBELLA SYNDROME • - Common congenital defects are deafness, cardiac malformations, cataracts, glaucoma, retinopathy, microcephalus, cerebral palsy, IUGR, hepato – splenomegaly and mental and motor retardation. • The first trimester of pregnancy infection affects the fetus and newborn baby with congenital defects, > abortion, stillbirth, PDA, cataract and deafness
- 39. PREVENTION • Active immunization with live attenuated vaccine. • RUBELLA VACCINE: 1979 – RA 27/3 vaccine (human diploid fibroblast) – produces higher antibody titer with good immune response. • Administration in a single dose 0.5 ml S.C • Sero conversion occurs in more than 95% vaccinees. Immunity persists for 14-16 yrs. • Infant should not be vaccinated. • Pregnancy – is contra indication for immunization. • Recipients of the vaccine should be advised not to become pregnant for next 3 months
- 40. Vaccination strategy • Combined vaccine MMR. VACCINATION STRATEGY: • - First to protect women of child bearing age (15-34/39) • Then interrupt transmission of rubella by vaccinating all children 1-14 yrs. • Subsequently all children at one-year age.
- 41. 41 Prevention of Rubella Immunization • Rubella vaccine: RA 27/3 strain,0.5 ml, SC,Life long immunity in 95% • C/I for immunization: Pregnancy • Recipients of vaccine should be advised not to become pregnant in 3 months after getting vaccine • MMR vaccine
- 42. 42 Vaccination strategy for Rubella • First protect women in 15-39 yr age • Second interrupt transmission by vaccinating children aged 1-14 years • Third, all children at age 1
- 45. 45 Global Measles and Rubella Strategic Plan 2012-2020 In 2012, the M&R Initiative launched a new Global Measles and Rubella Strategic Plan which covers the period 2012-2020. • By the end of 2015 the plan aims: to reduce global measles deaths by at least 95% compared with 2000 levels; • To achieve regional measles and rubella/congenital rubella syndrome (CRS) elimination goals. • By the end of 2020 the plan aims: to achieve measles and rubella elimination in at least 5 WHO regions.
- 46. 46 The strategy focuses on the implementation of 5 core components: • Achieve and maintain high vaccination coverage with 2 doses of measles- and rubella-containing vaccines; • Monitor the disease using effective surveillance, and evaluate programmatic efforts to ensure progress and the positive impact of vaccination activities; • Develop and maintain outbreak preparedness, rapid response to outbreaks and the effective treatment of cases; • Communicate and engage to build public confidence and demand for immunization; and • Perform the research and development needed to support cost- effective action and improve vaccination and diagnostic tools.