Download to read offline




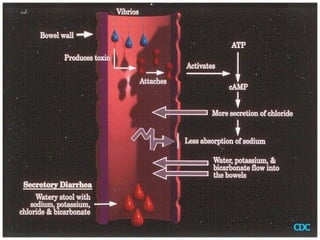

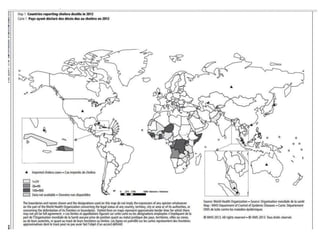













Cholera is an acute diarrheal disease caused by the bacterium Vibrio cholerae. It remains a global threat, with an estimated 2.9 million cases and 95,000 deaths worldwide annually. The disease spreads through contaminated food and water and can kill within hours if left untreated. Cholera outbreaks typically occur in areas with poor sanitation and lack of clean drinking water. Prevention relies on vaccination, water treatment, hygiene and proper sanitation.






























![Cholera Disease hya 2[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/choleradiseasehya21read-only-230528122422-1de77771-thumbnail.jpg?width=640&height=640&fit=bounds)











![Cholera[1]...........................pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cholera1-250108134552-35c9c003-thumbnail.jpg?width=640&height=640&fit=bounds)











































