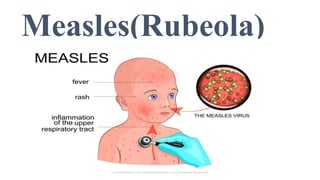
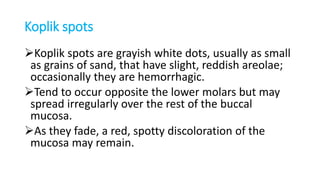
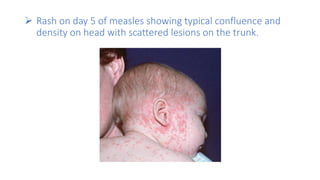
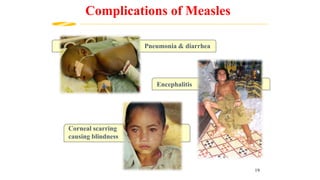
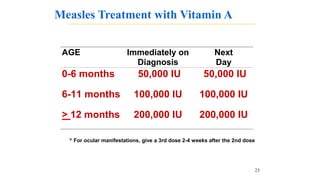
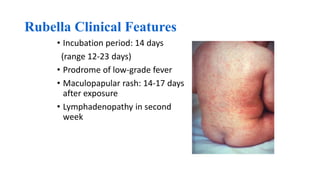
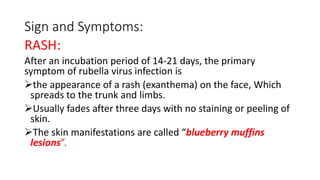
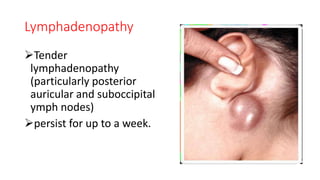
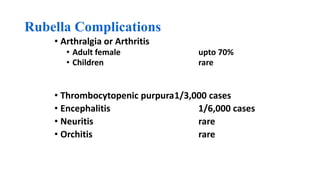
This document provides information on measles and rubella. For measles, it describes the causative virus, signs and symptoms including the pathognomonic Koplik spots, complications such as pneumonia and encephalitis, and treatment including vitamin A supplementation. It also compares measles and chickenpox rashes. For rubella, it discusses the virus, transmission, clinical features including rash and lymphadenopathy, complications in adults and congenital rubella syndrome in infants, and prevention through vaccination of children.