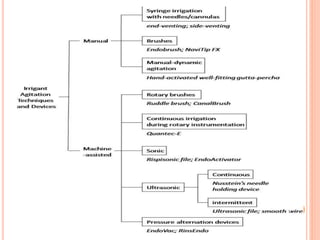
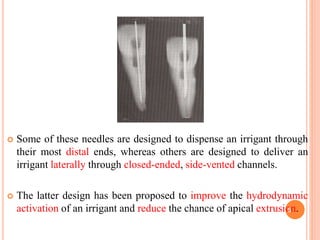
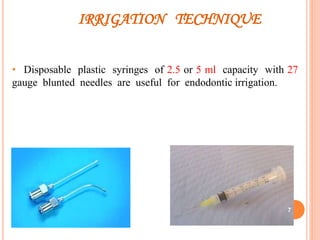
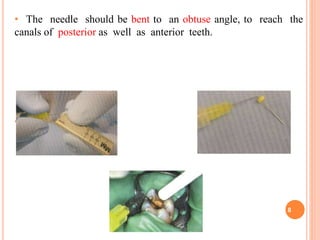
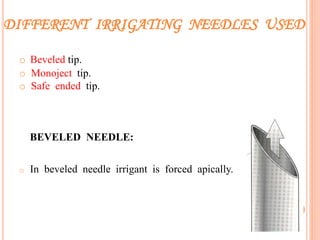
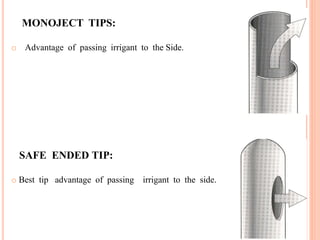

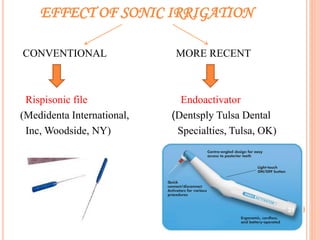
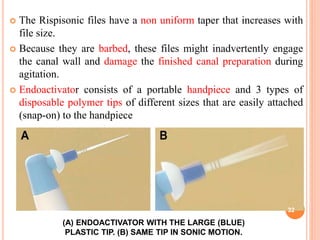

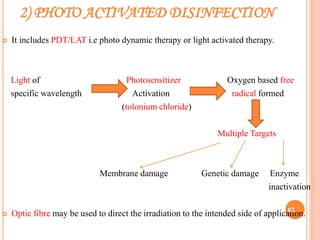


This document summarizes recent advances in irrigation devices used in endodontics. It describes both manual and machine-assisted irrigation techniques. For manual techniques, it discusses syringe irrigation with different needle types, use of brushes, and manual dynamic irrigation. It also covers machine-assisted devices like rotary brushes, continuous irrigation during instrumentation, sonic irrigation with devices like the Rispisonic file and Endoactivator. The document provides details on how each technique works and its advantages over other methods.


































































