

















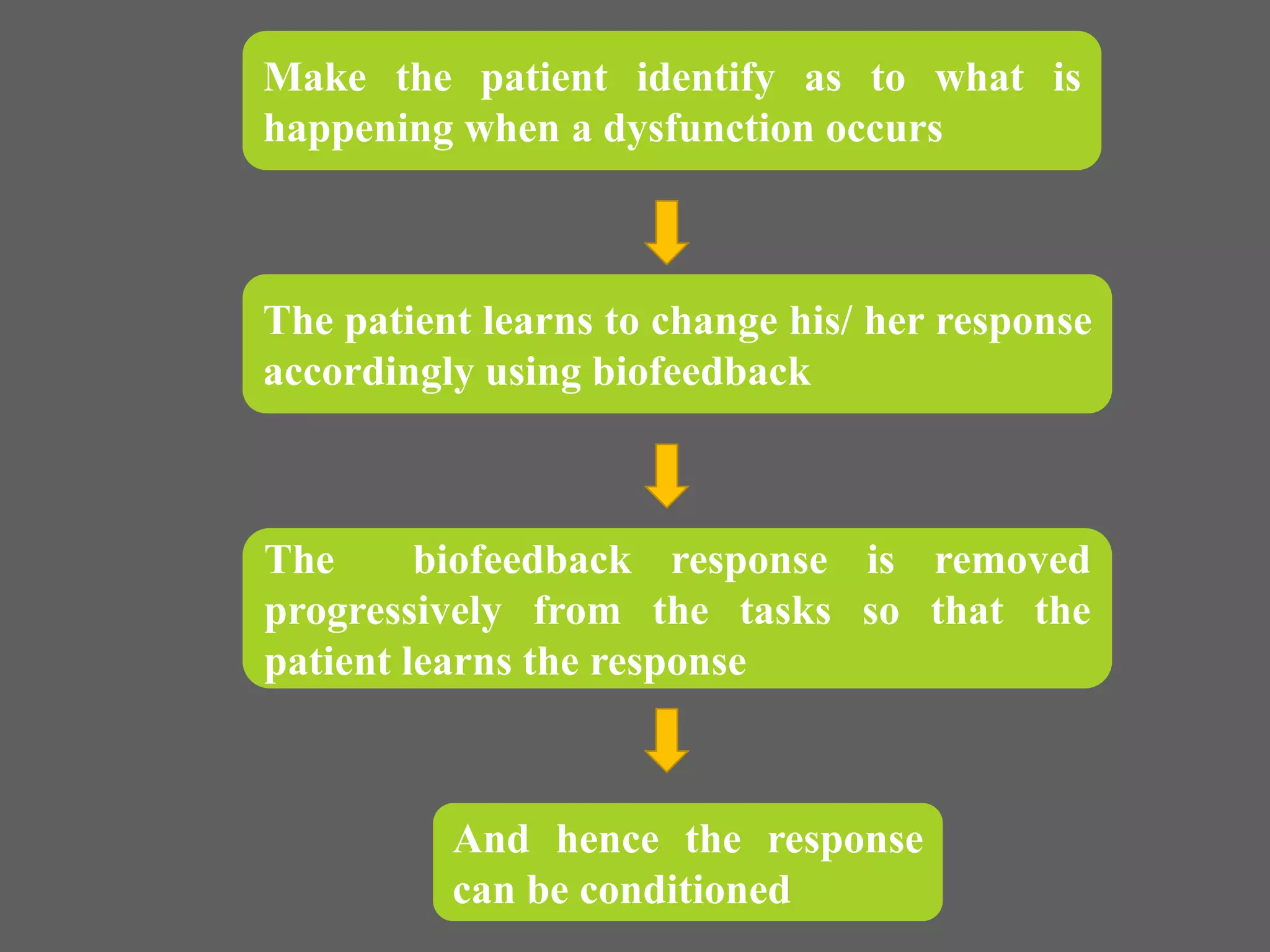

























The document discusses biofeedback, including its definition, purpose, mechanisms, and clinical use. Biofeedback aims to make internal physiological processes more visible using instrumentation in order to help patients gain control over these processes. It works by initially making patients aware of sensations during dysfunctions and conditioning alternative responses. Successful biofeedback requires selecting appropriate feedback signals, starting at achievable levels and gradually increasing requirements as control improves through shaping behavior.




































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)


















