

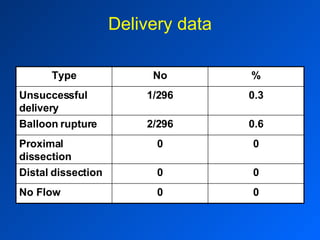
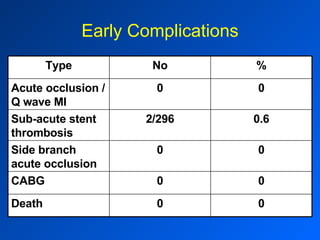
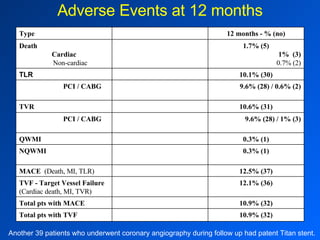
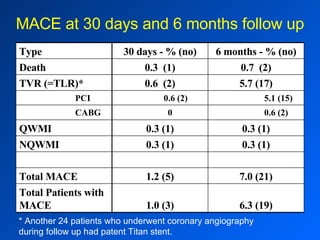
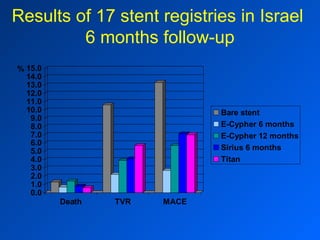



This document summarizes the results of a multi-center registry assessing the short and long term outcomes of using the Titan stent in 296 patients. Some key findings include: - At 6 months follow-up, the rates of target vessel failure and major adverse cardiac events were 10.9% and 12.1% respectively. - The rates of target lesion revascularization at 30 days and 6 months were 0.6% and 5.7% respectively. - The Titan stent demonstrated a good safety profile with no deaths within 30 days and a cardiac death rate of 1% at 6 months. - The results compare favorably to other stent registries conducted in Israel.




























































































