

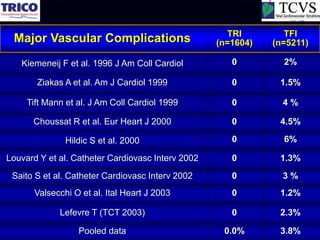
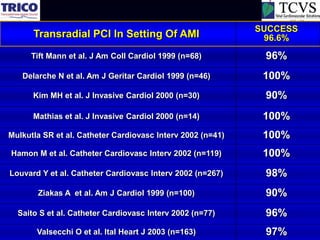
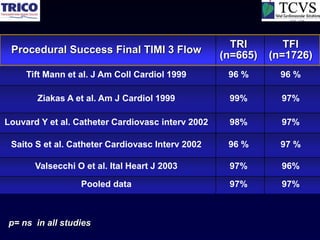
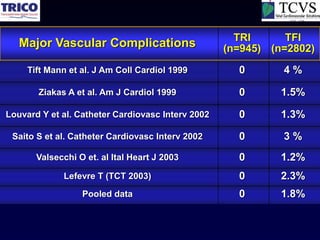
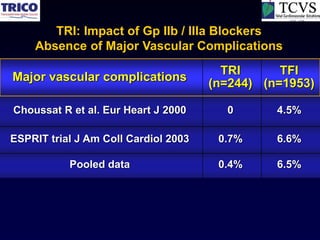
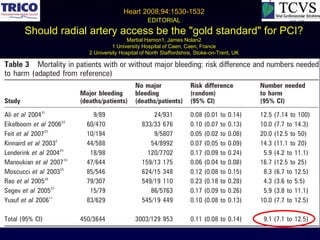
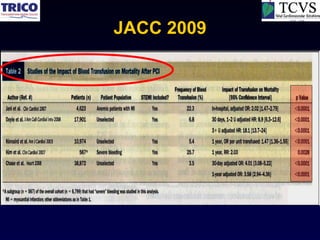
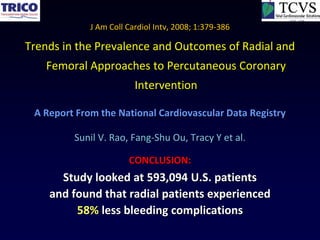
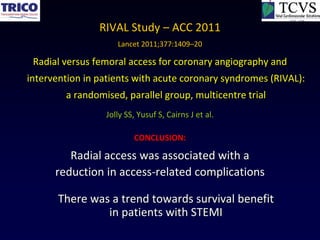






































Transradial approach for coronary procedures has several advantages over transfemoral approach: 1) It virtually eliminates major vascular complications such as bleeding, which can significantly reduce mortality. 2) Multiple randomized controlled trials and meta-analyses have shown transradial approach reduces major bleeding without compromising procedural success or delaying reperfusion times. 3) The reduced bleeding leads to fewer blood transfusions, which are associated with increased mortality. Therefore, transradial approach may provide a survival benefit.























































































