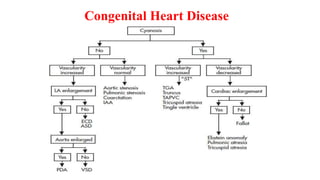
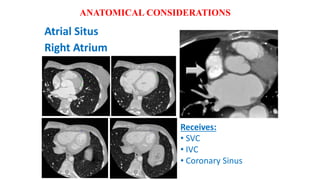
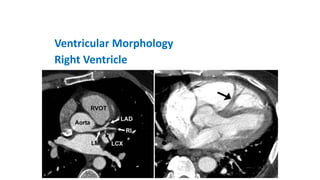
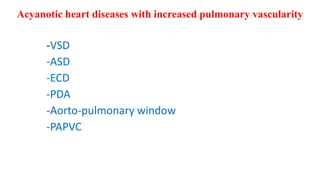
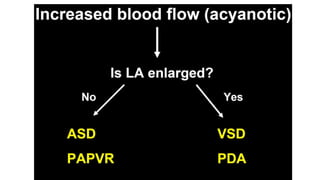
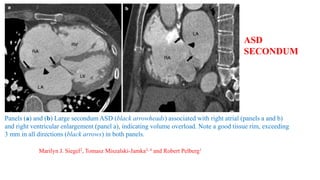
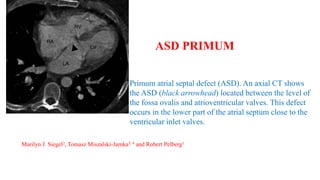
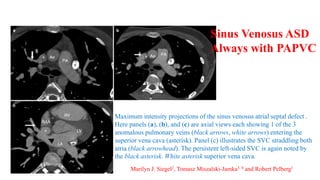
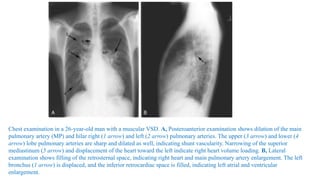
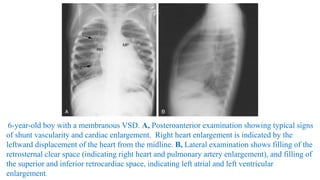
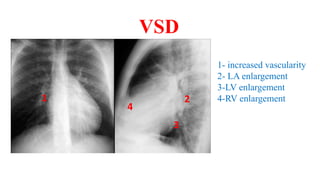
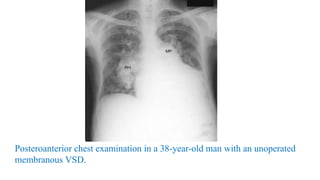
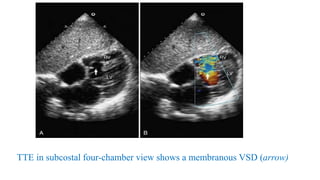
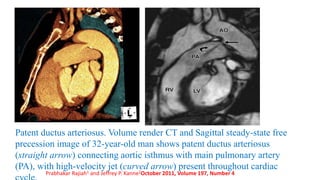
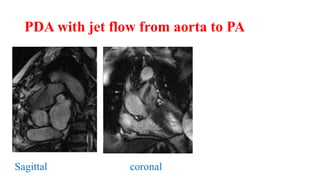
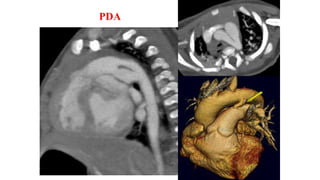
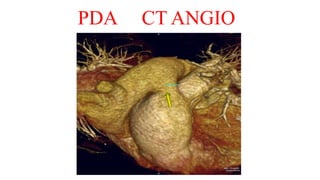
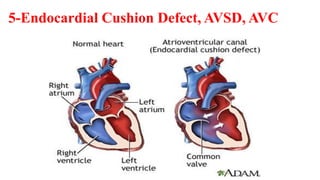
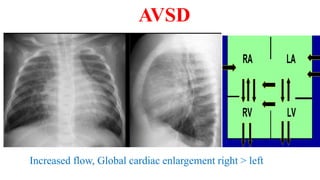
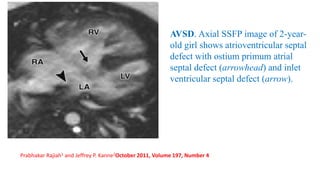
The document discusses imaging of congenital heart diseases, describing the main types of defects such as atrial septal defects (ASD), ventricular septal defects (VSD), and patent ductus arteriosus (PDA). It provides details on the anatomy, classifications, imaging findings, and clinical presentations of each type of defect. Examples of echocardiograms and chest x-rays are shown to illustrate the imaging appearance of various congenital heart abnormalities.
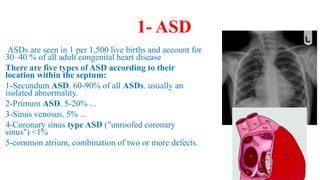



















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
