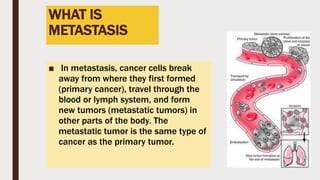
Metastatic bone lesions occur when cancer cells spread from the original tumor site to the bones. The skeleton is one of the most common sites of cancer metastasis, after the liver and lungs. Bone metastases can cause severe pain, fractures, and other complications. Treatment options aim to reduce symptoms and improve quality of life, and may include radiation therapy, medication such as bisphosphonates, chemotherapy, surgery, and pain management.