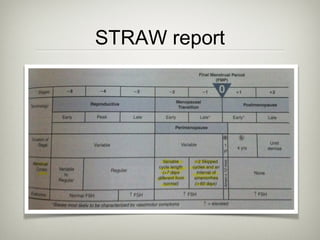
This document provides an overview of menopause, including definitions, physiological changes, diagnosis, and treatments. It discusses the average age of menopause and influential factors. It defines menopause, premature ovarian failure, and the menopausal transition period. It then covers changes to the hypothalamus-pituitary-ovarian axis, ovaries, endometrium, central thermoregulation, and other areas. It provides details on evaluating abnormal uterine bleeding and discusses treatment options like hormone replacement therapy, antidepressants, clonidine, gabapentin, and complementary therapies.

![PTH response
• ↓ Ca intake or gut absorption ➔ low [ca] serum
• ↓ [Ca] ➔ ↑ production of PTH
• ↑ PTH = ↑ bone resorption to ↑ [Ca]
• Premenopausal pt : after ↑ in Ca, PTH quickly
return to N
• Postmenopausal pt : greater response to PTH *](https://image.slidesharecdn.com/menopausecopy-joannie-131120161655-phpapp01/85/Menopause-copy-joannie-77-320.jpg)


![Memory
• Henderson et al (2007) reanalyzed data from the
WHIMS trial:
• All-cause dementia was significantly less likely to
develop in women reporting prior HT
• Women’s Estrogen for Stroke Trial Estrogen
administrated for troke prevention
• No impact of E Tx, except in women with normal
function at baseline, who had less decline in
cognitive domains (RR, 0.46 [95% CI, 0.24 to 0.87])](https://image.slidesharecdn.com/menopausecopy-joannie-131120161655-phpapp01/85/Menopause-copy-joannie-150-320.jpg)