Downloaded 14 times



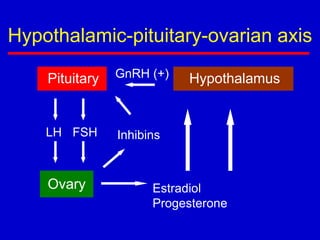





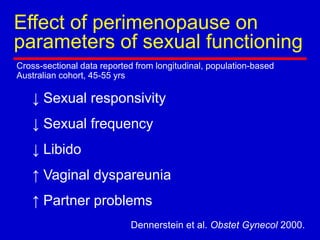


Menopause is defined as the permanent cessation of menstruation resulting from loss of ovarian activity, occurring naturally or induced by surgery or medications. It typically occurs between ages 45-55. The document discusses the hypothalamic-pituitary-ovarian axis and changes that occur during perimenopause and menopause, including symptoms. Evaluation of menopausal women includes assessments of risk factors, symptoms, and quality of life to guide lifestyle and medical management options.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



