Downloaded 71 times
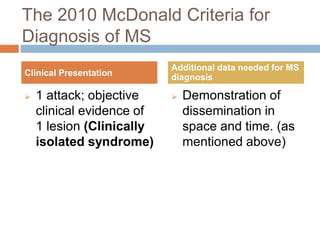
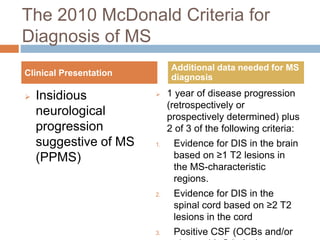
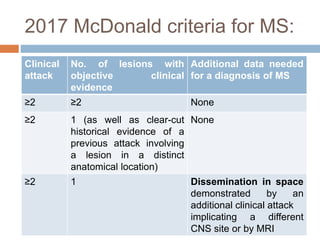
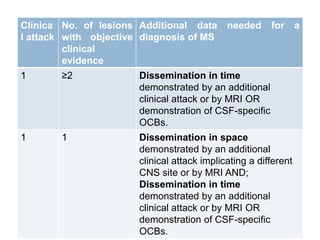


This document summarizes the revisions made to the McDonald criteria for diagnosing multiple sclerosis over time. The 2017 revisions aimed to simplify and clarify the 2010 criteria to facilitate earlier diagnosis when MS is likely but not definitively diagnosed. Key changes include allowing symptomatic and asymptomatic lesions to demonstrate dissemination in space and time, and cortical/juxtacortical lesions to fulfill MRI criteria. CSF oligoclonal bands alone can now establish a diagnosis. The revisions were motivated by new data on diagnostic accuracy in diverse populations and distinguishing MS from similar conditions.



































































