Download to read offline




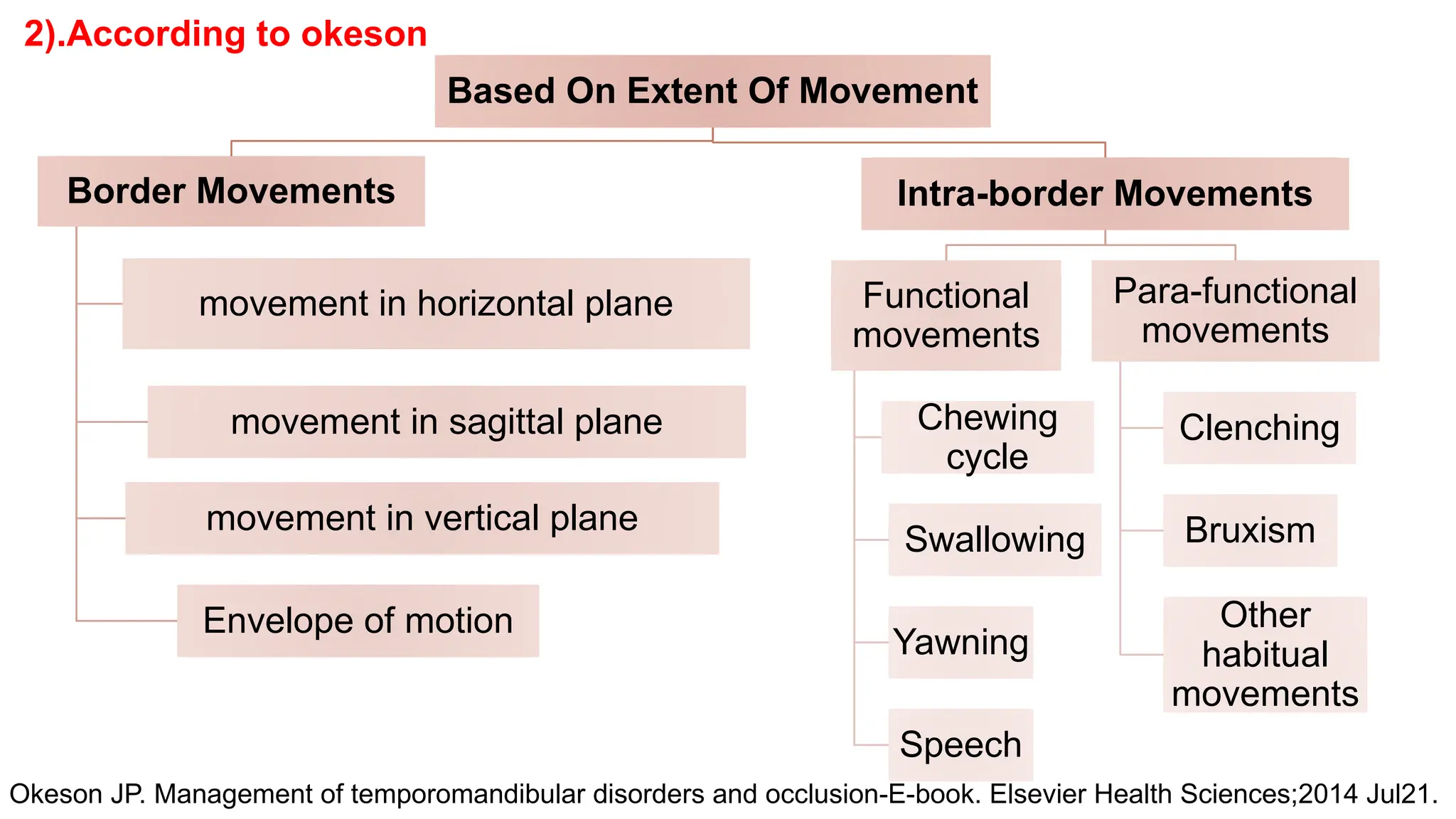


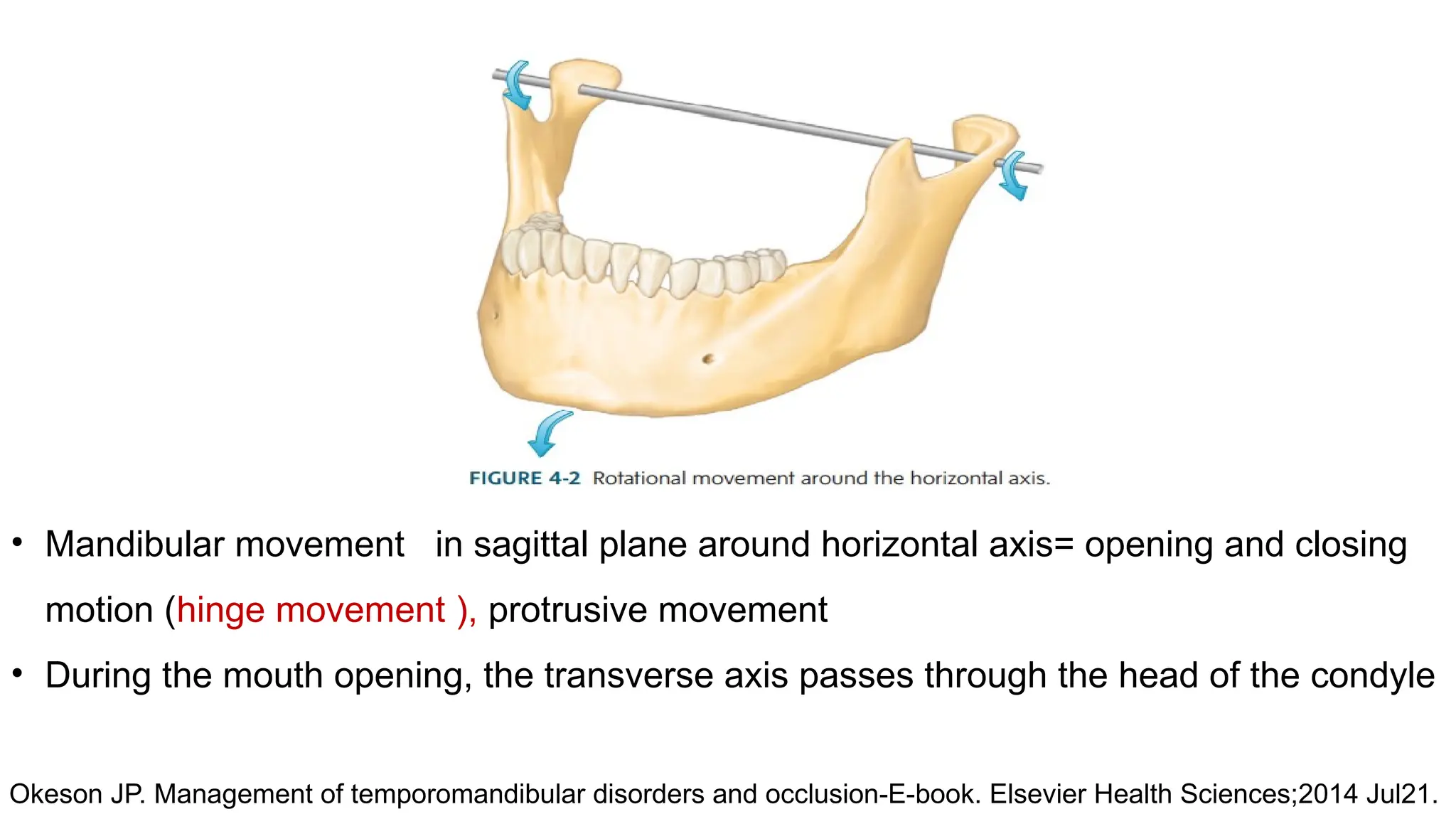





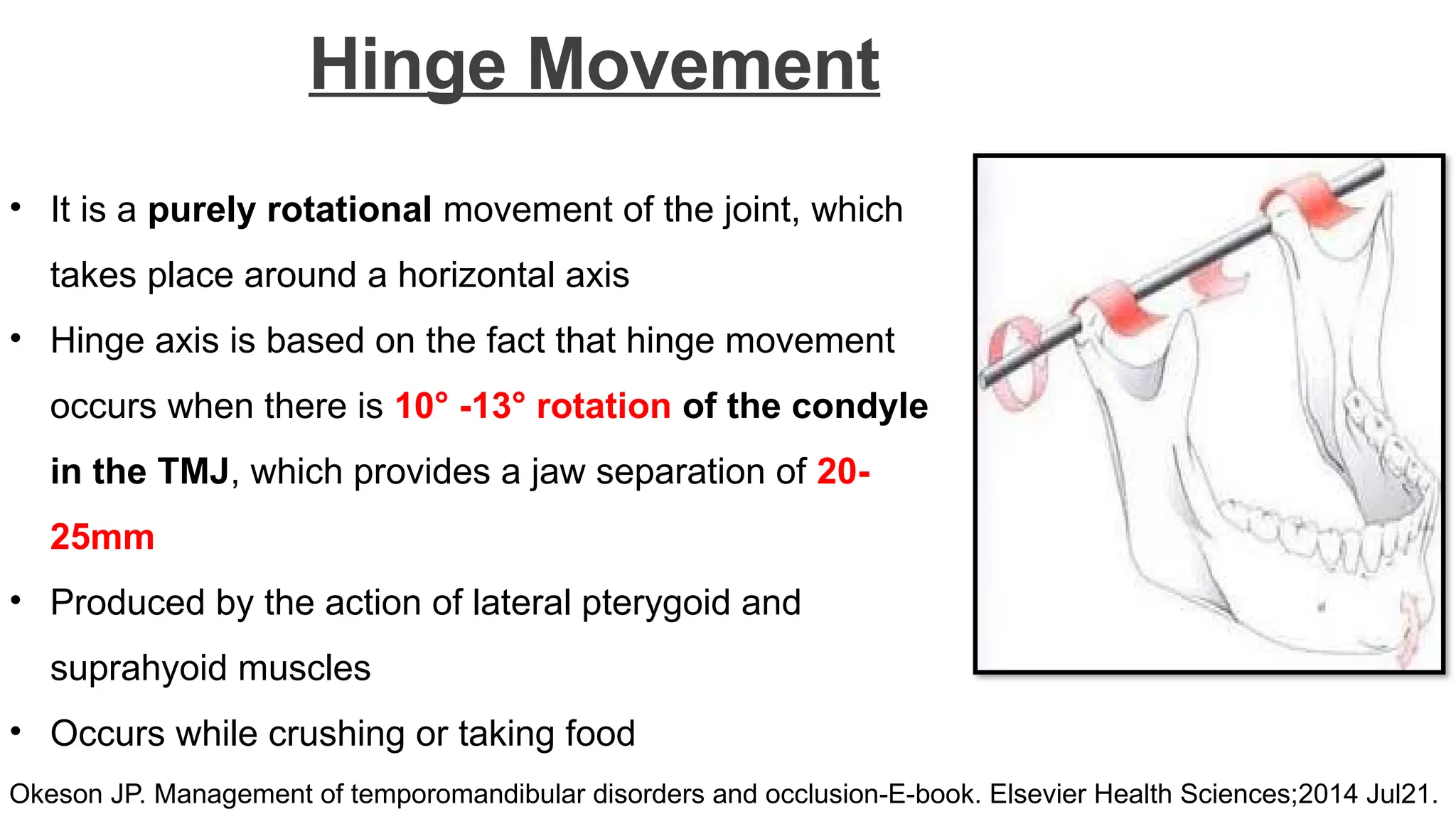



































































Introduction Classification Hinge movement Protrusive and Retrusive movement Lateral movement Border movements in Sagittal plane Border movements in Horizontal plane Border movements in Vertical plane Envelope of Motion Functional and parafunctional movement Importance of Mandibular Movements Summary References Introduction Classification Hinge movement Protrusive and Retrusive movement Lateral movement Border movements in Sagittal plane Border movements in Horizontal plane Border movements in Vertical plane Envelope of Motion Functional and parafunctional movement Importance of Mandibular Movements Summary References Introduction Classification Hinge movement Protrusive and Retrusive movement Lateral movement Border movements in Sagittal plane Border movements in Horizontal plane Border movements in Vertical plane Envelope of Motion Functional and parafunctional movement Importance of Mandibular Movements Summary References Introduction Classification Hinge movement Protrusive and Retrusive movement Lateral movement Border movements in Sagittal plane Border movements in Horizontal plane Border movements in Vertical plane Envelope of Motion Functional and parafunctional movement Importance of Mandibular Movements Summary References #MandibularMovements #TMJAnatomy #DentalSeminar #OcclusionMatters #JawKinetics #FunctionalDentistry #TMJDisorders #JawMovements #OralPhysiology #ProsthodonticsBasics












































































