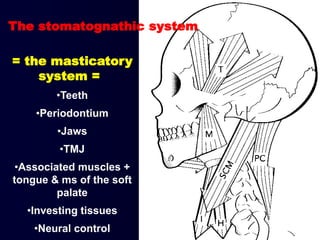
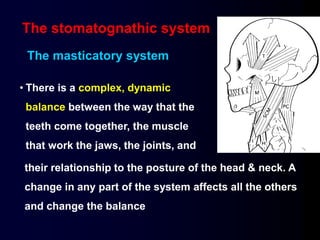
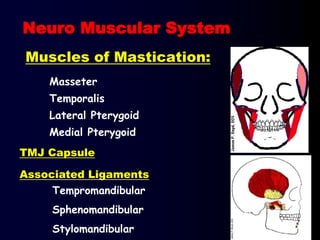
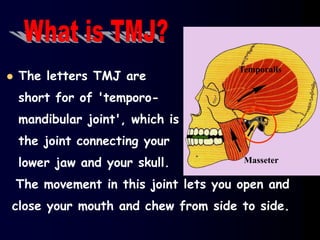
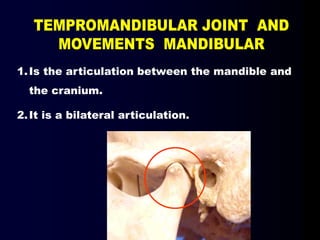
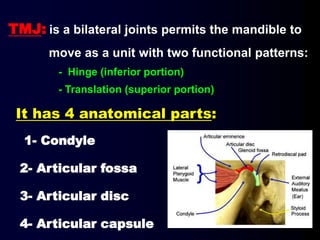
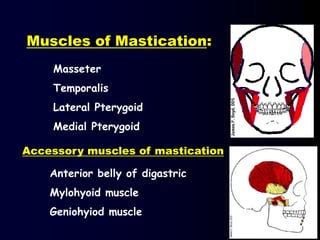
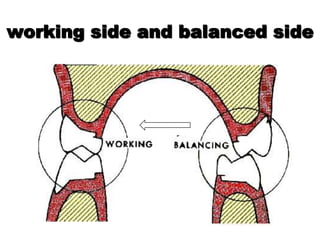
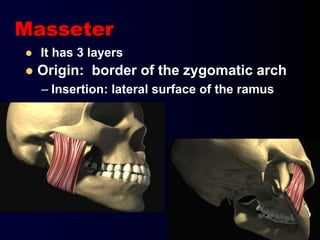
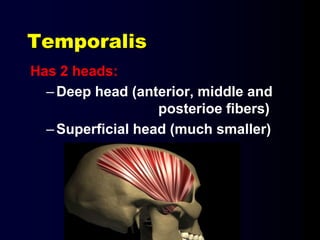
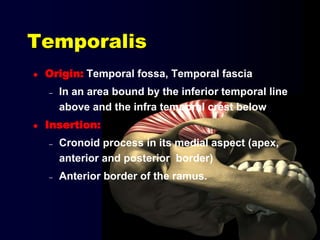
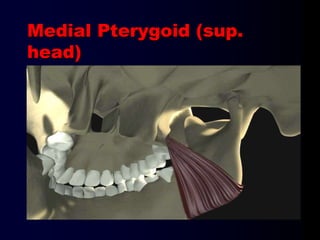
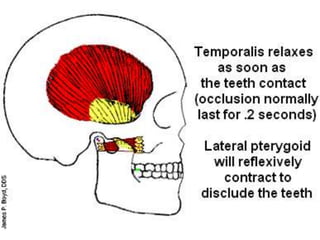
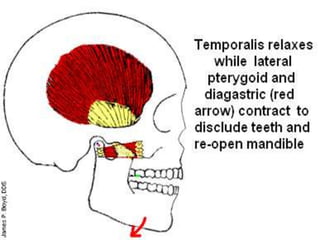
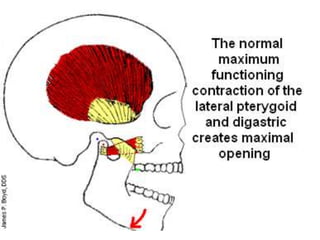
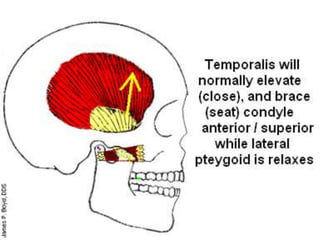
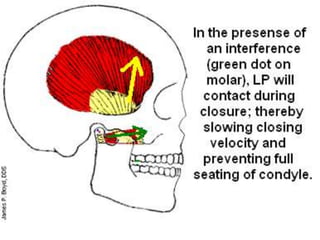
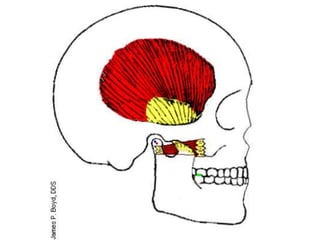
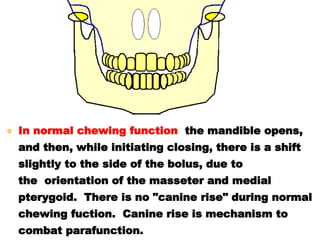
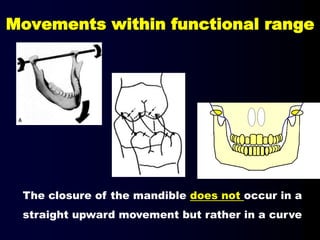
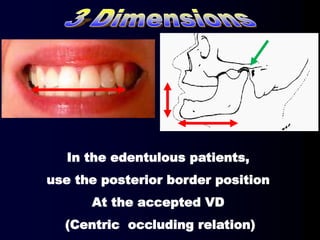
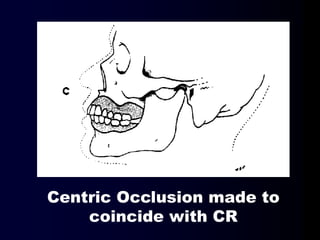
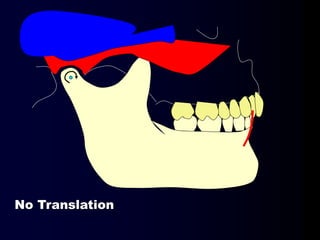
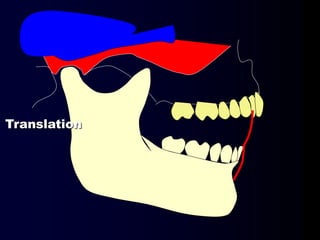
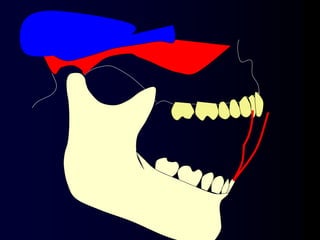
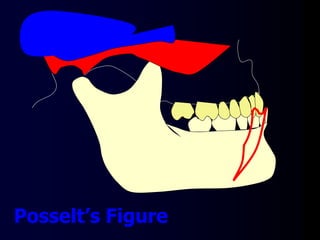
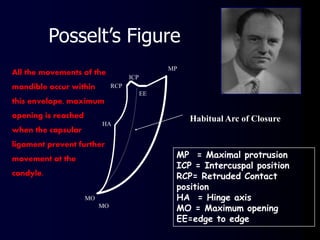
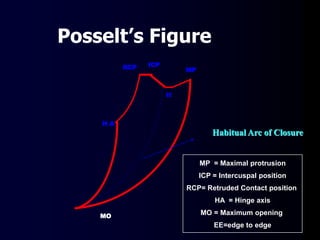
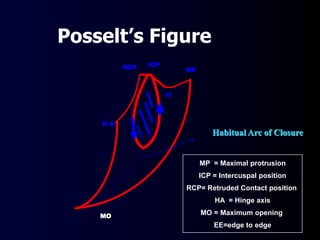
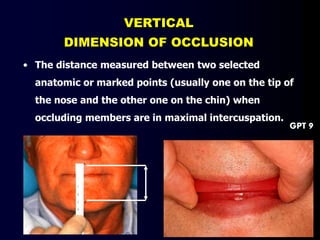
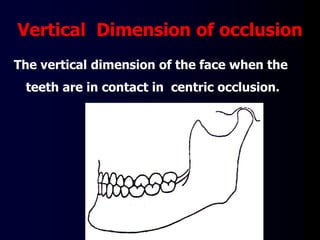
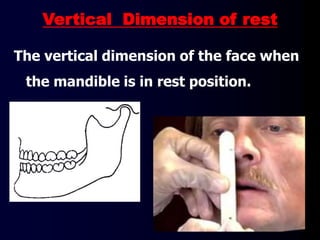
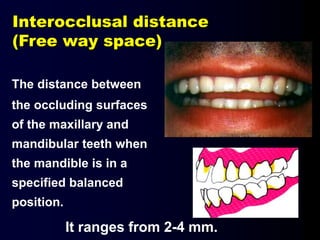
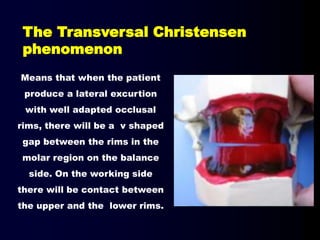
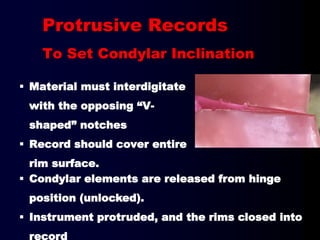
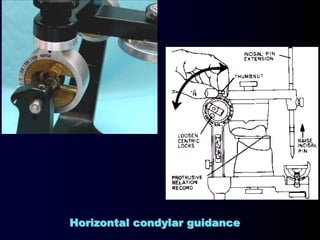
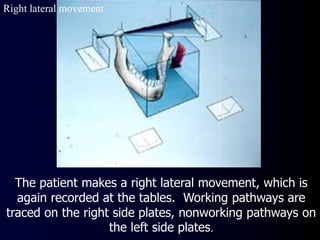
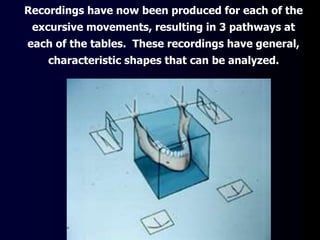
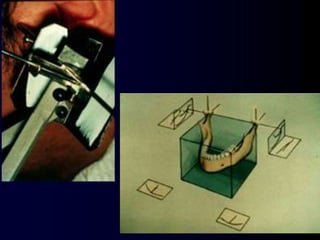
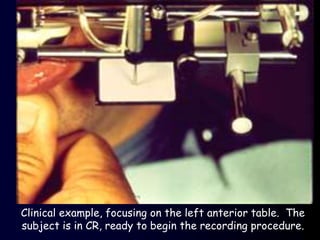
The document outlines the complex interactions within the stomatognathic system, including the importance of occlusion, mandibular movements, and the roles of various muscles and joints such as the temporomandibular joint (TMJ). It details key components like the masseter and pterygoid muscles, their functions in mastication, and the relationships between different occlusal positions. Additionally, the text describes methods for recording occlusion and the significance of maintaining stability in the masticatory system.