Download as PDF, PPTX




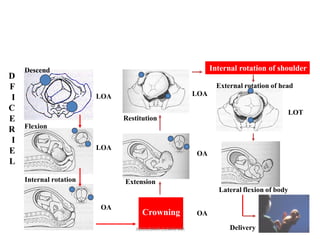
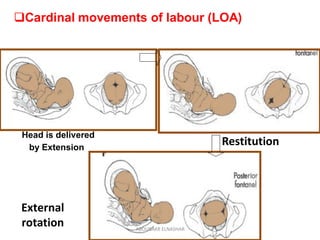
























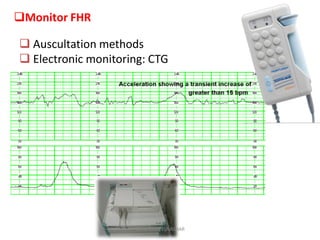
























































This document provides information on the management of normal labor. It defines labor and delivery and outlines the cardinal movements of labor. It discusses assessing and monitoring labor through the stages including fetal wellbeing, maternal wellbeing, and labor progress using a partogram. It covers managing each stage of labor including the first stage of dilation, the second stage of delivery, and the third stage of delivery of the placenta. Key points like positioning, pushing techniques, and care of the newborn are summarized.







































































































