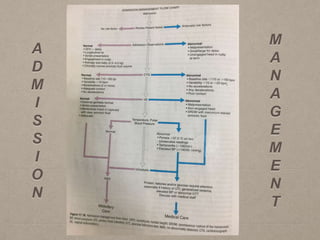
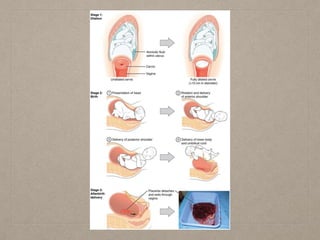
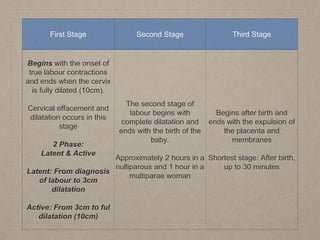
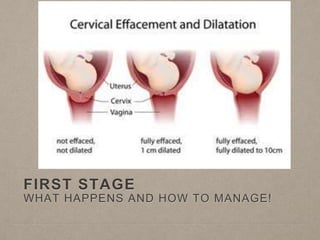
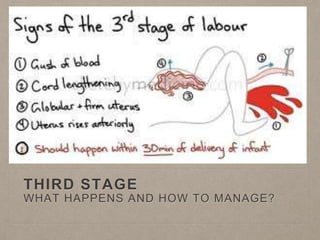
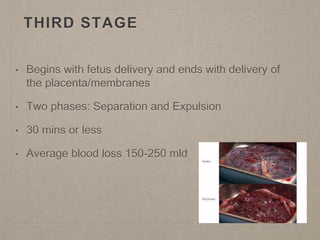
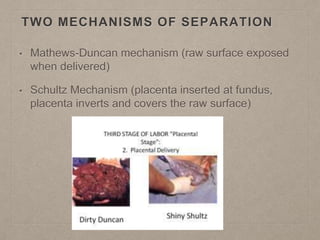
This document discusses normal labour and delivery. It defines normal labour and outlines the factors that influence the progress of labour, including the 3 P's - power (uterine contractions), passenger (fetus), and passageway (maternal pelvis). It then describes the stages of labour, including the first stage (cervical dilation), second stage (baby's delivery), and third stage (placental delivery). It provides details on managing each stage of labour and monitoring the mother and baby throughout the process.















![mechanism_of_labor[1].pptx obstetrics and gynaecology midwifery nursing mater...](https://cdn.slidesharecdn.com/ss_thumbnails/mechanismoflabor1-250610164745-6b6dfb9d-thumbnail.jpg?width=640&height=640&fit=bounds)






































