Download as PDF, PPTX
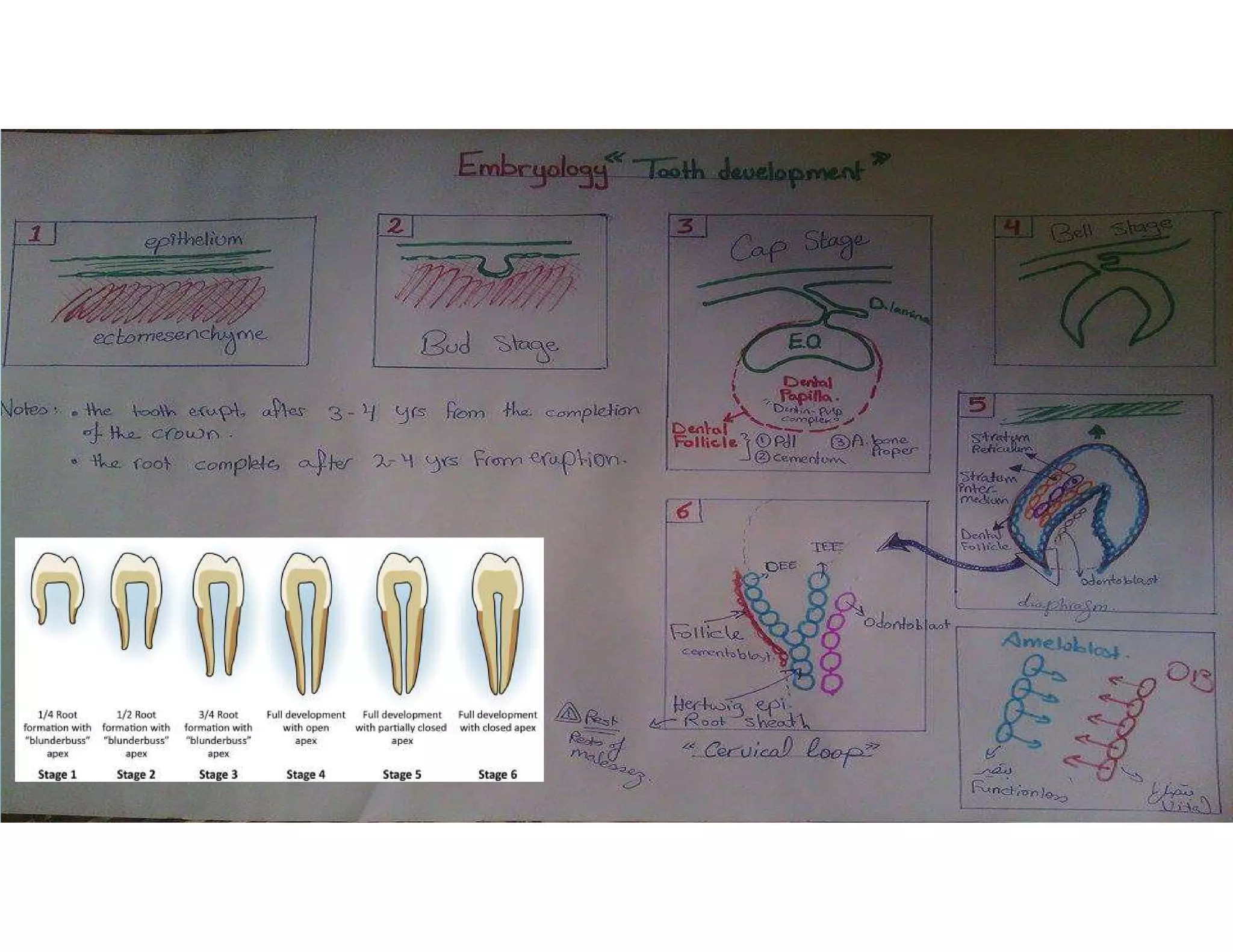
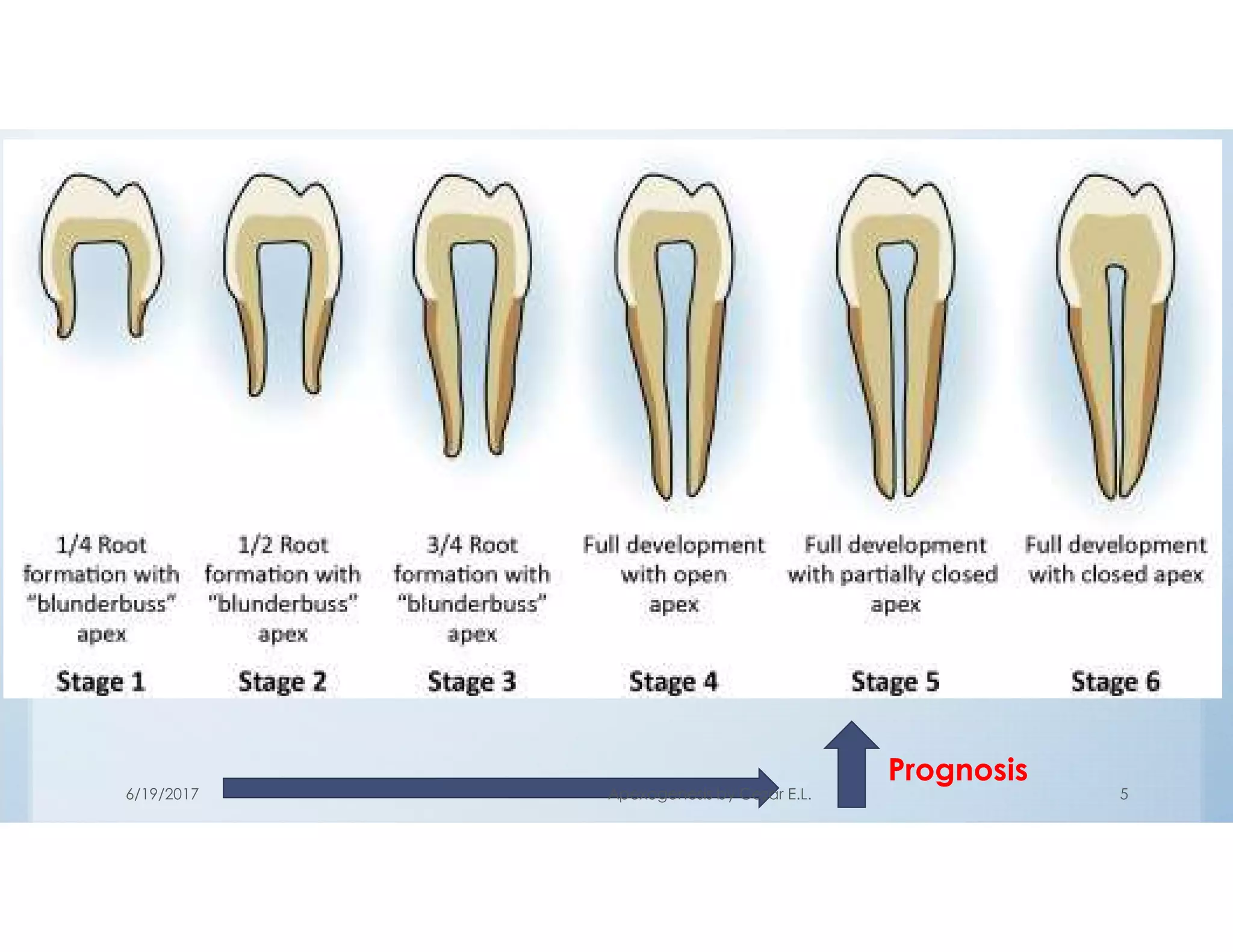



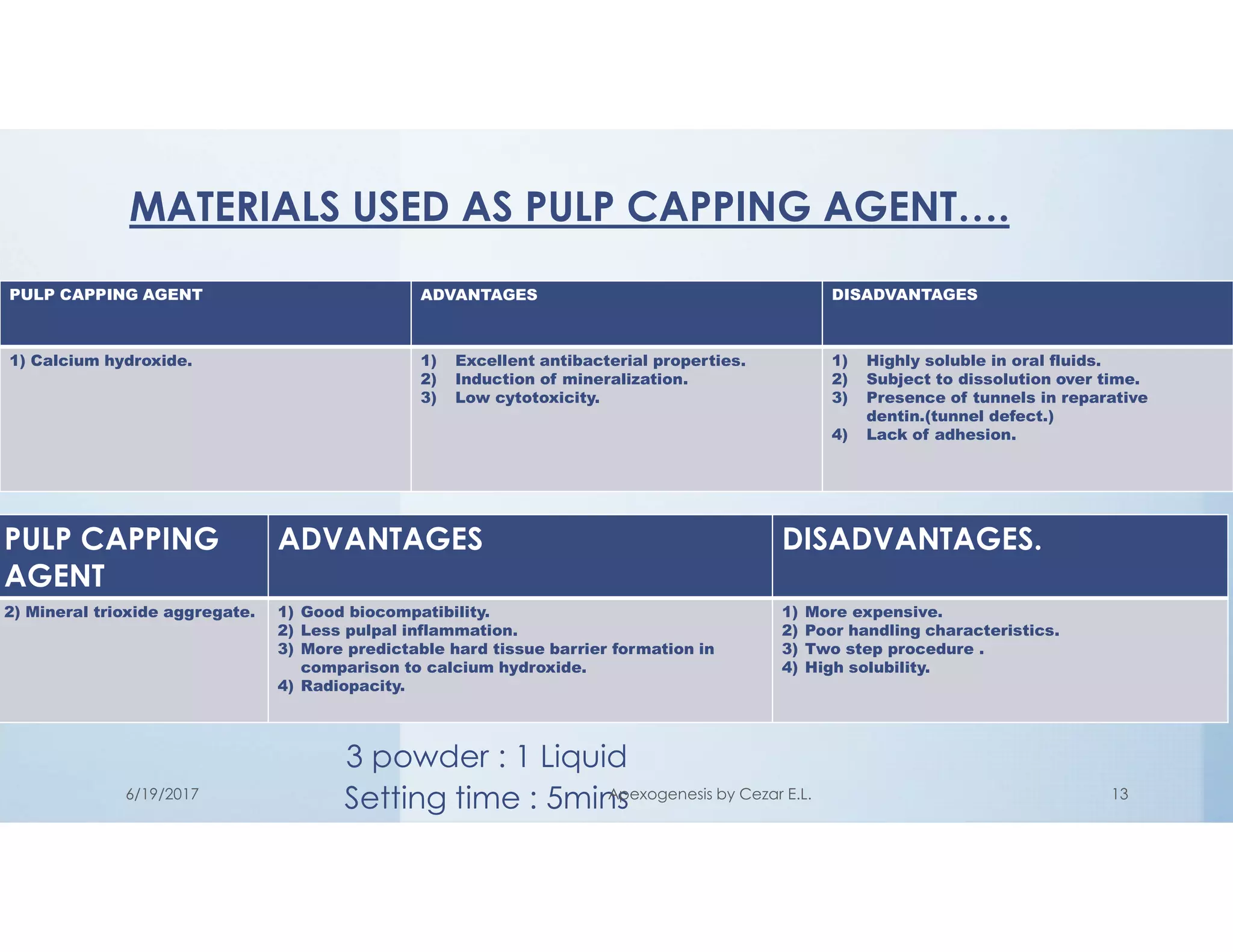
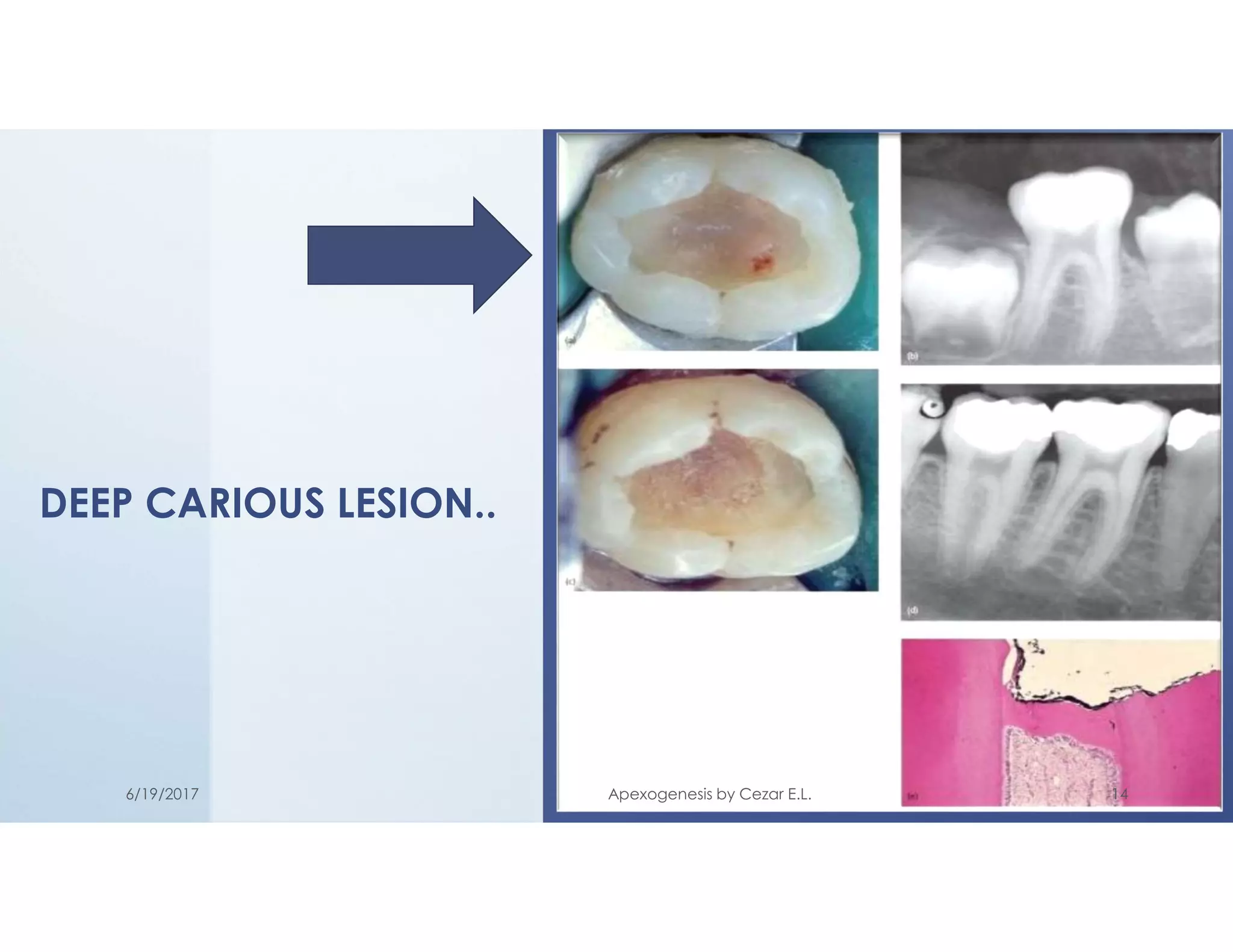
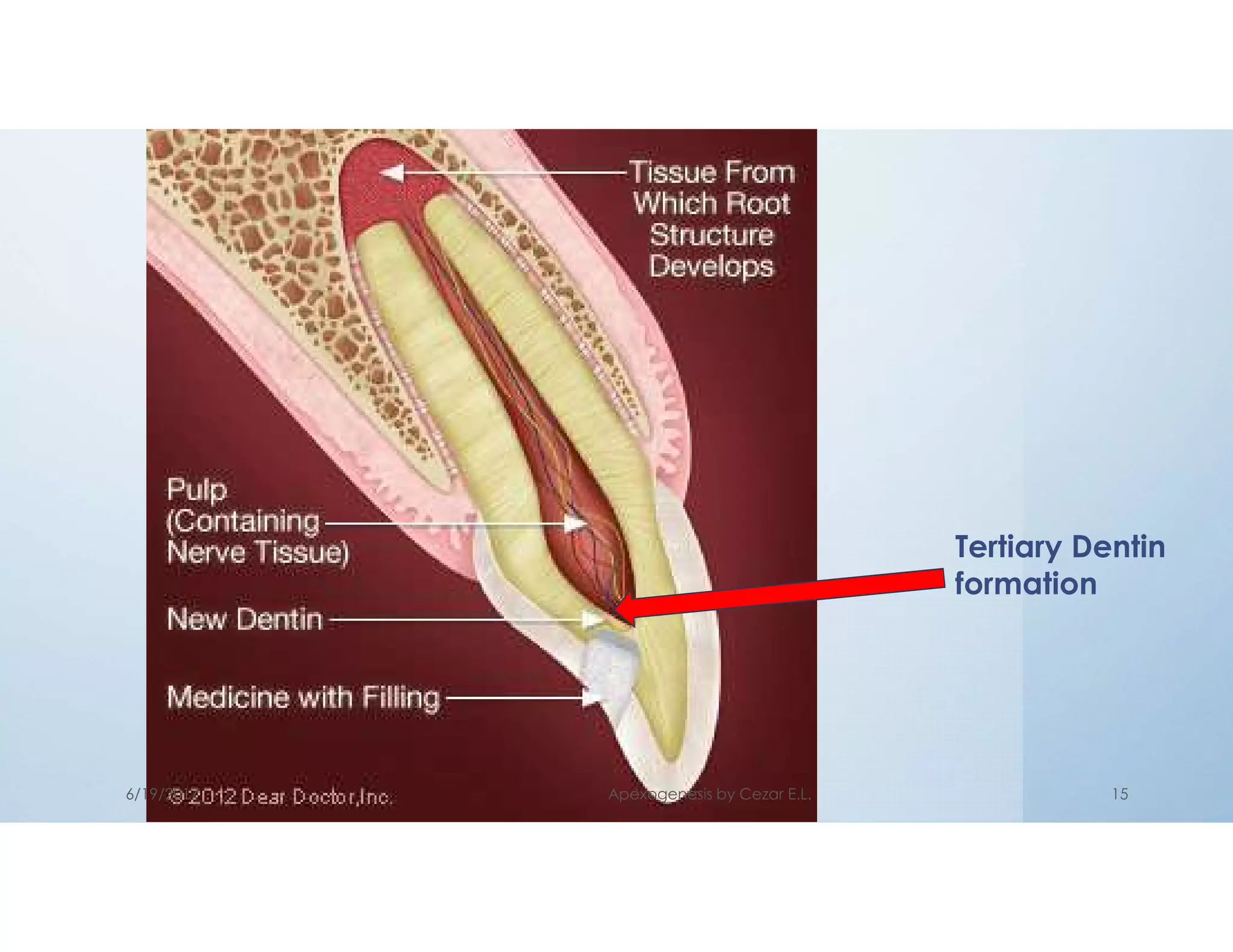
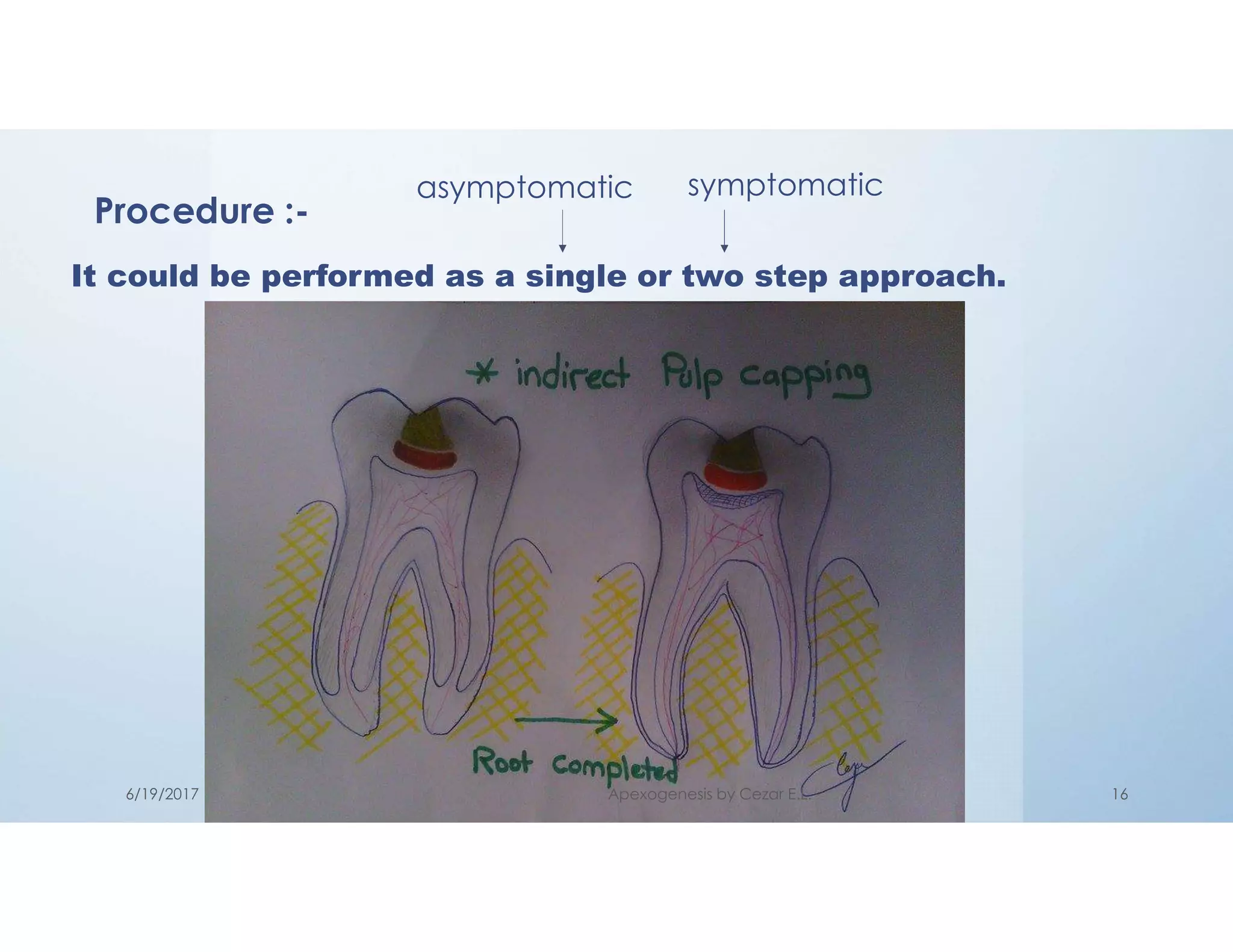


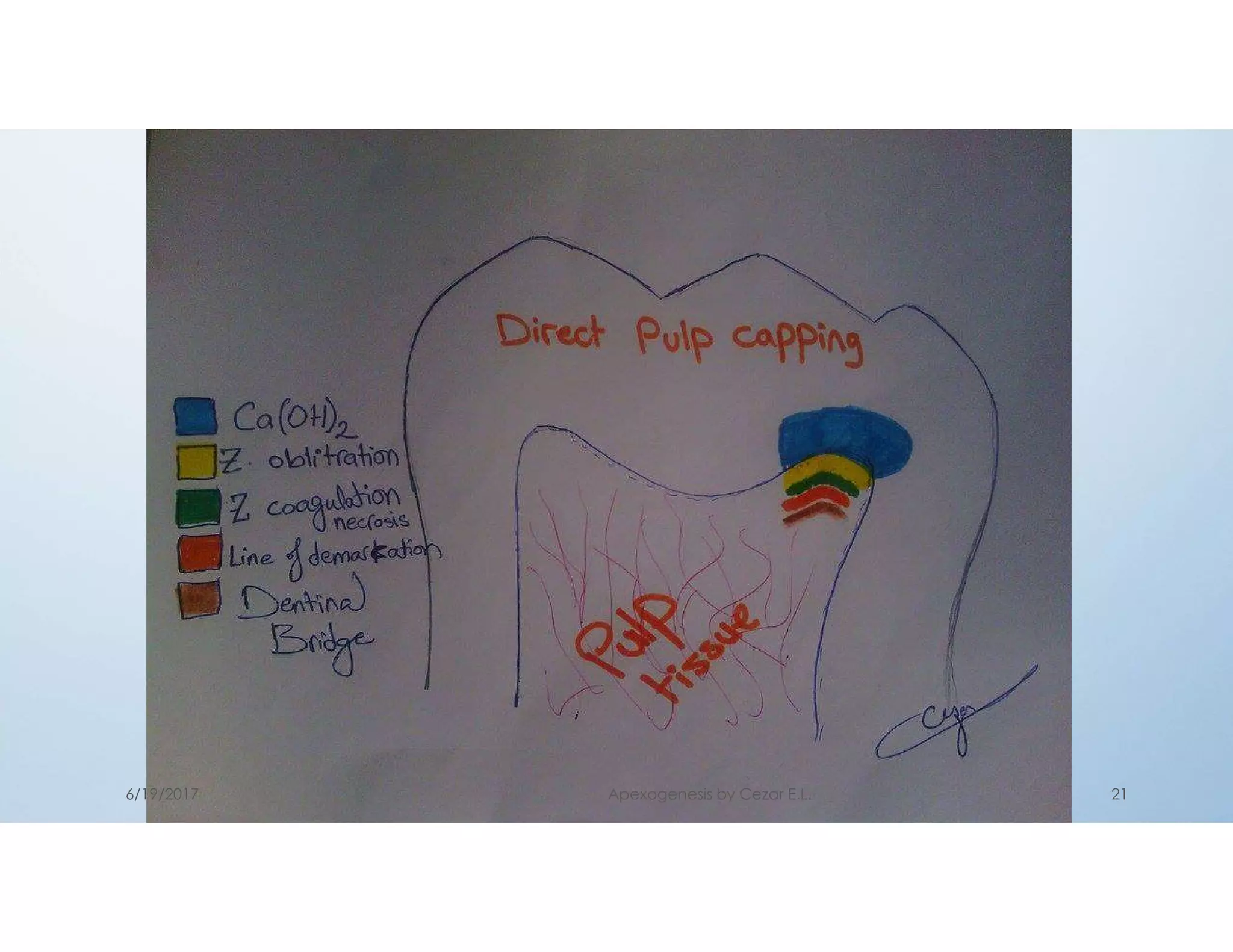
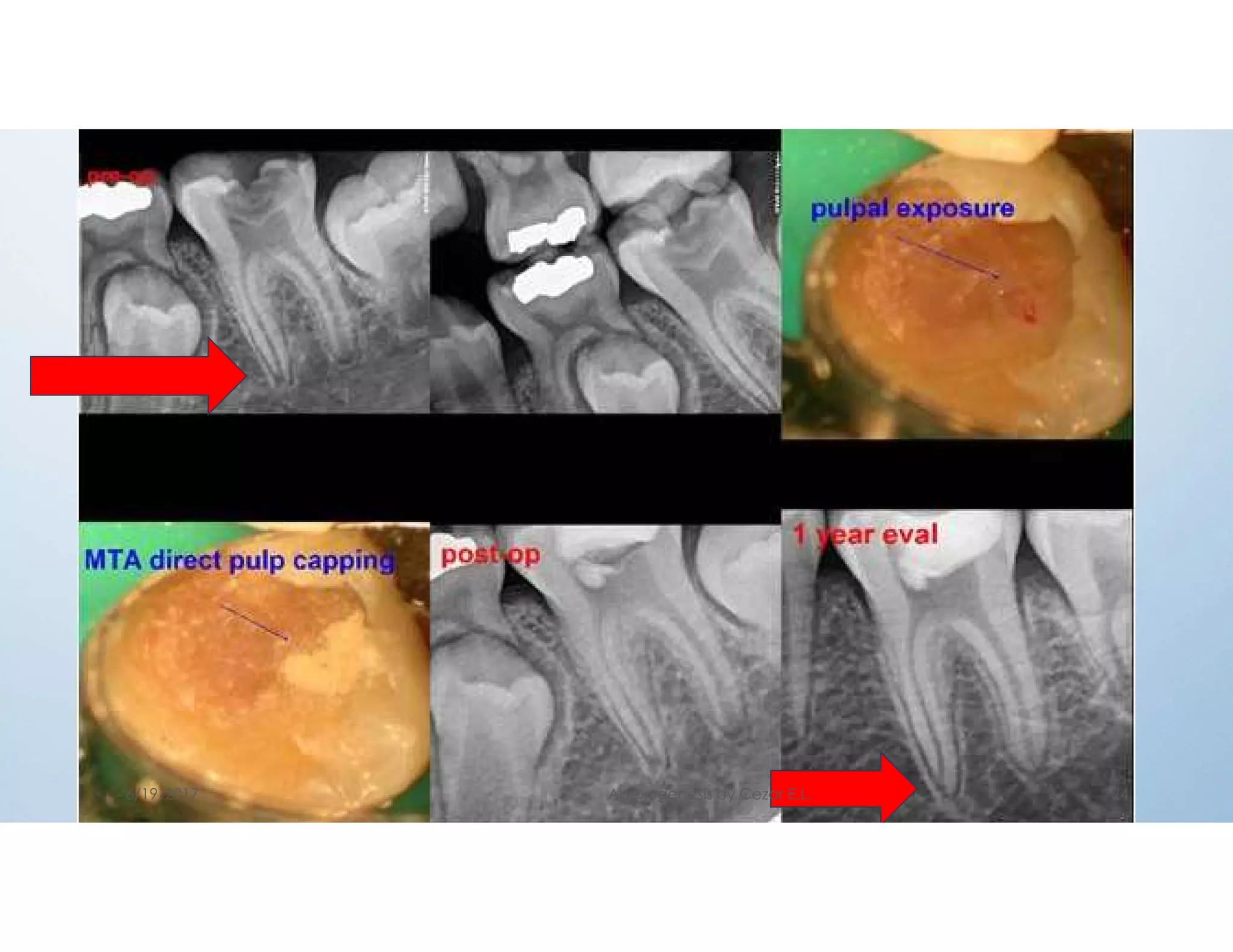



This document outlines the management of incomplete root formation in vital teeth. It discusses the embryology of tooth development, factors that can influence root development, and the goal of apexogenesis to promote continued root development and closure of the apex. Three techniques for apexogenesis are described: indirect pulp capping, direct pulp capping, and pulpotomy. For each technique, the definition, goals, indications, contraindications, materials used, and procedure are explained. Calcium hydroxide and MTA are highlighted as common medicaments used. Successful outcomes of apexogenesis include continued root development, a calcified barrier over the radicular pulp, and maintenance of pulp vitality and normal responses to testing.























































































