
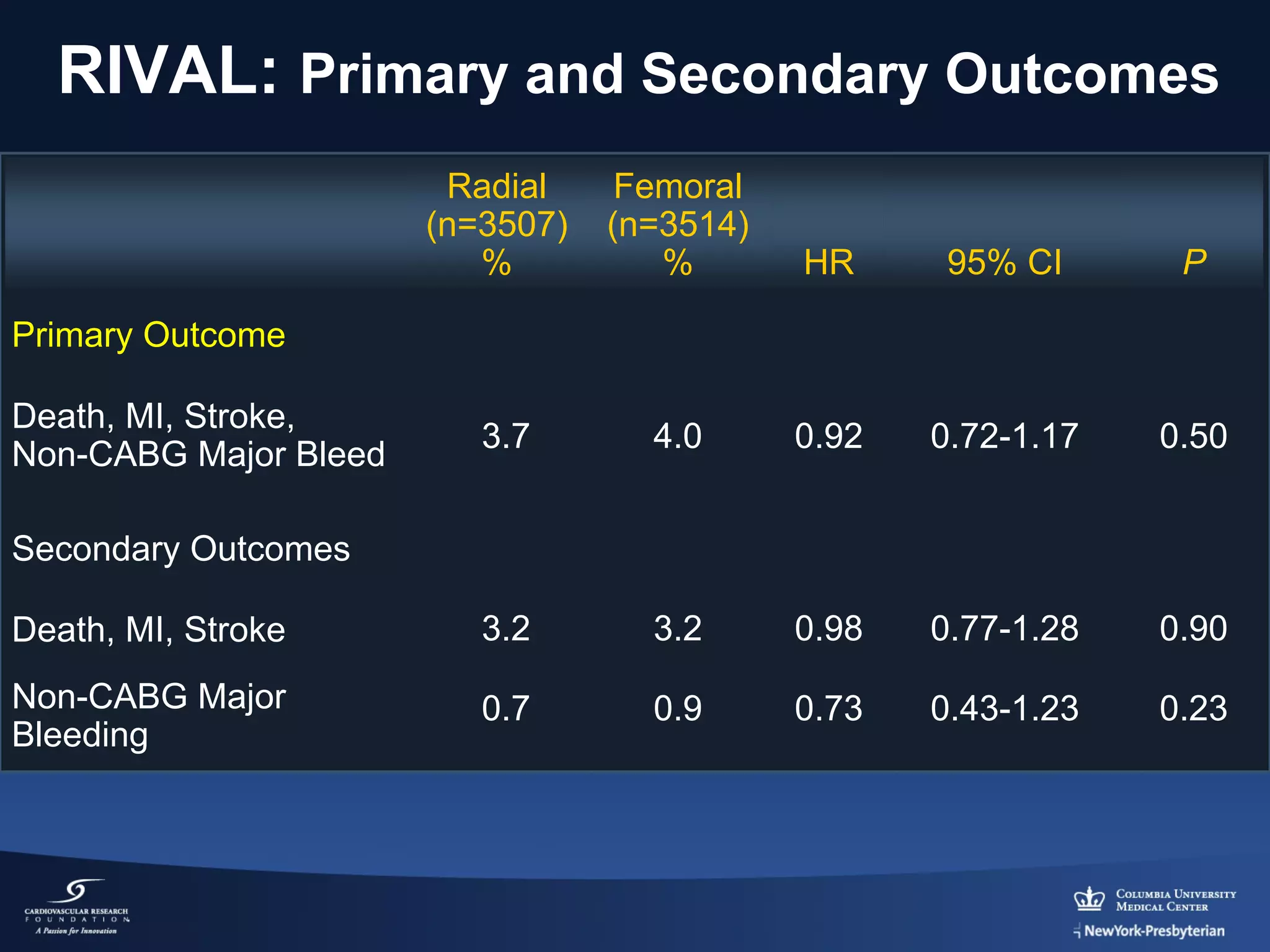
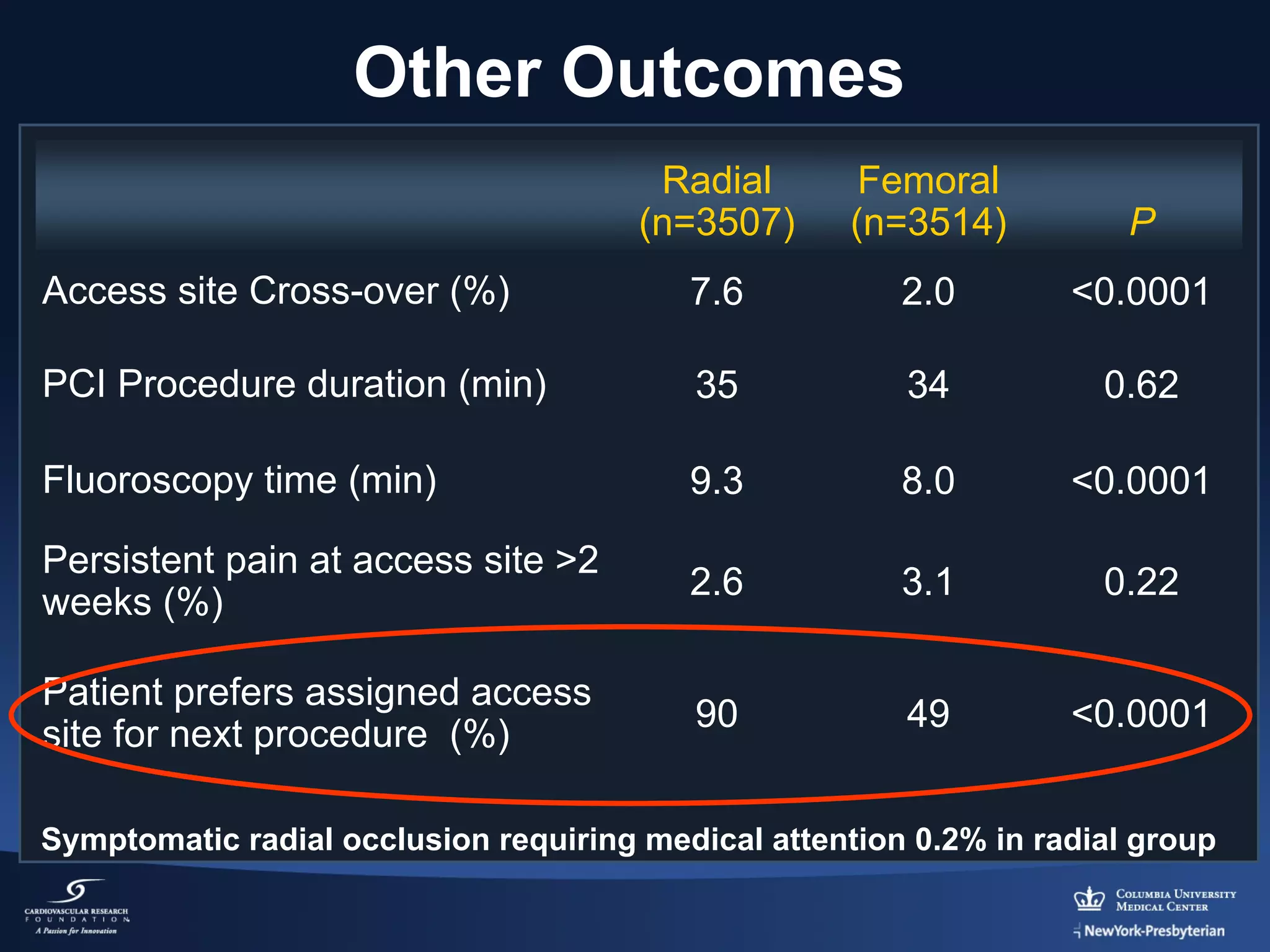
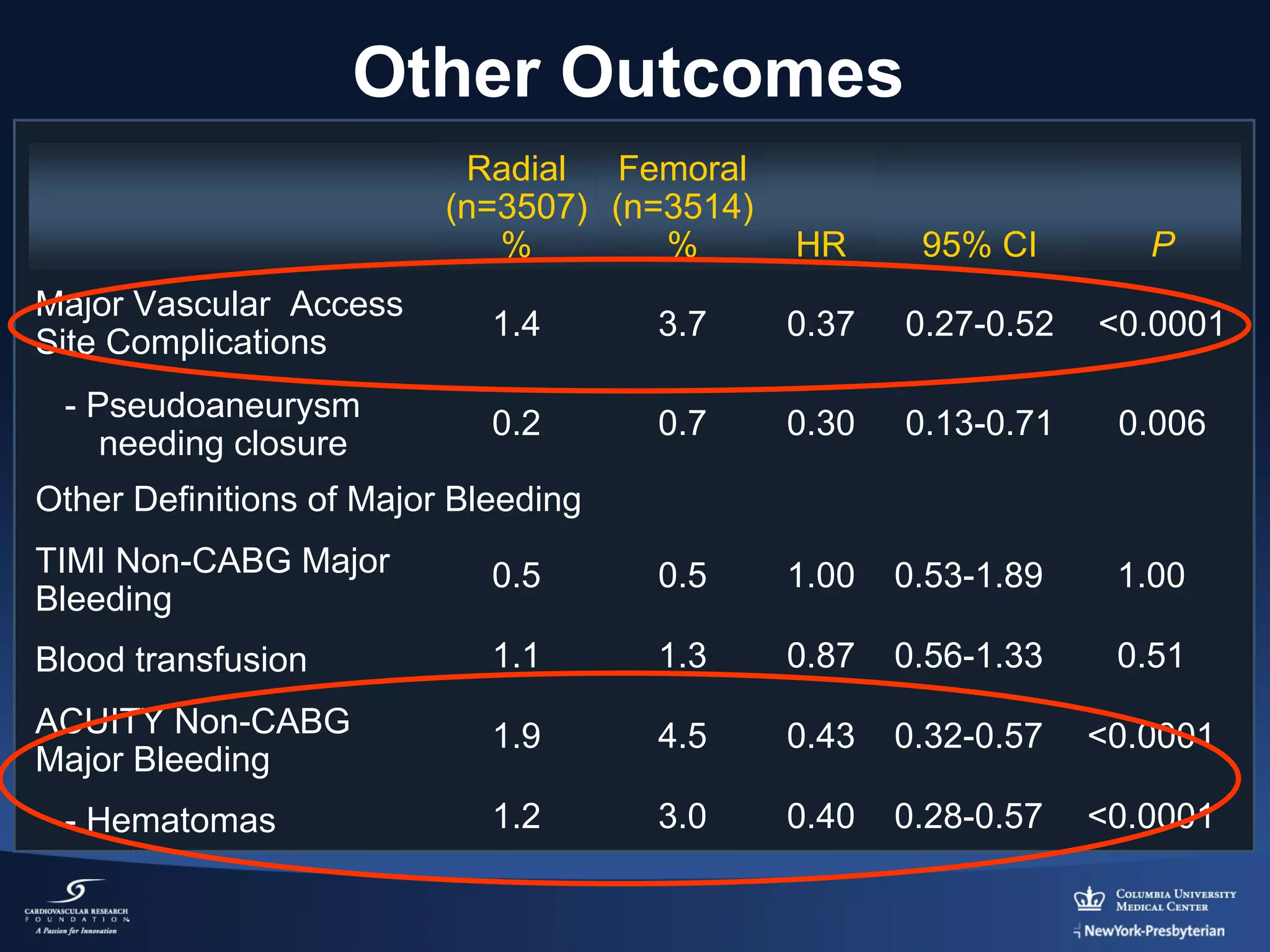
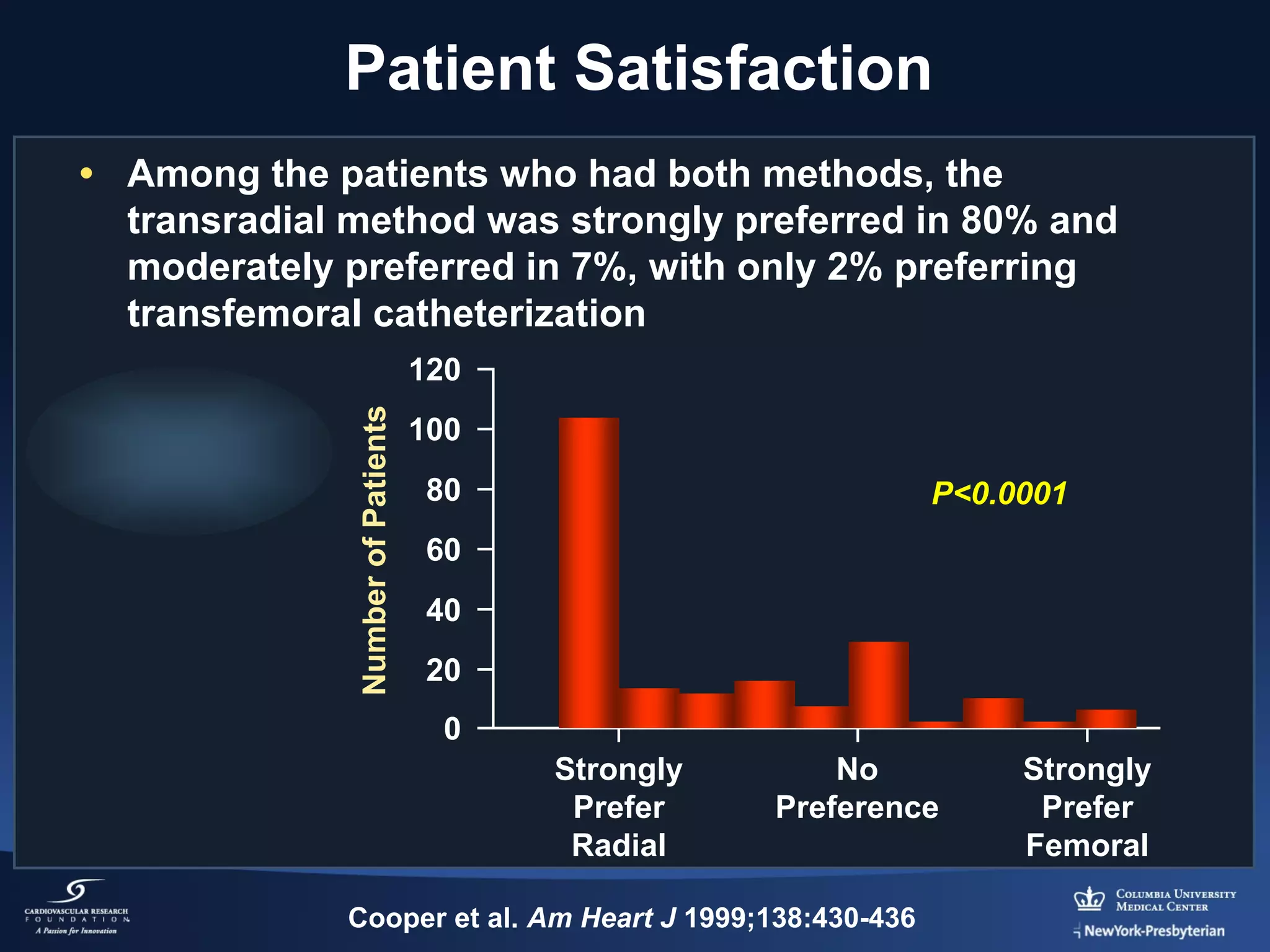

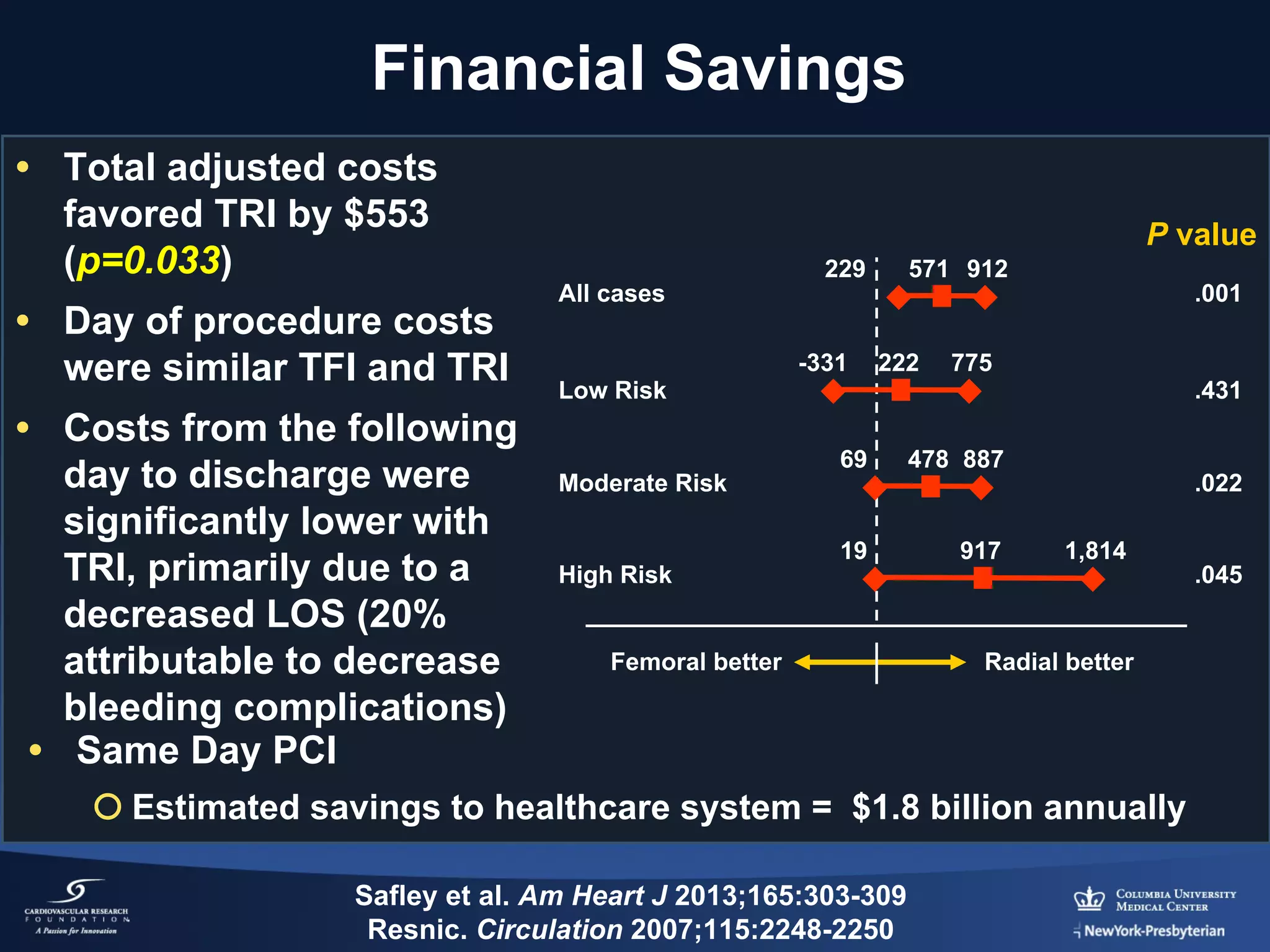
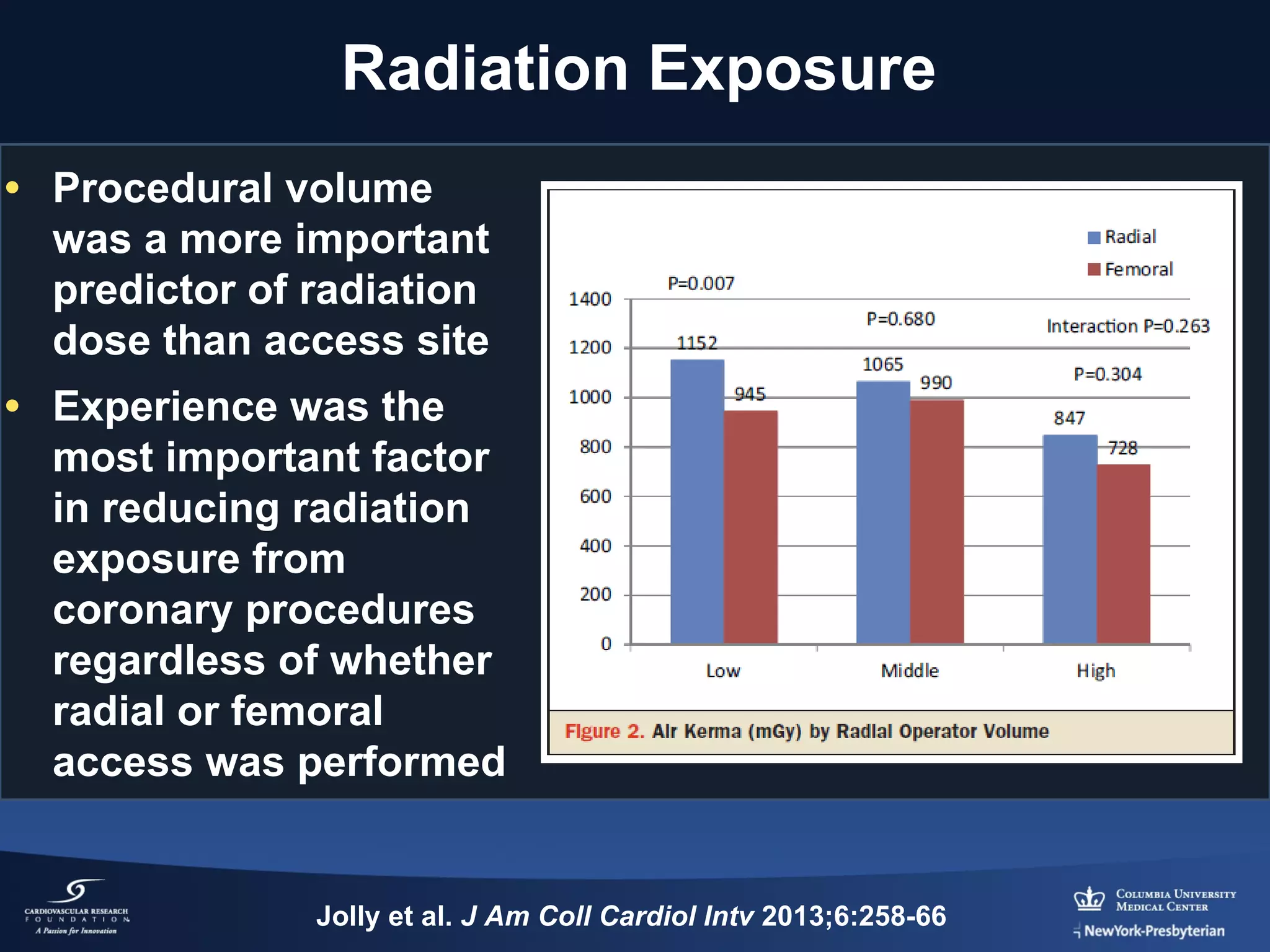
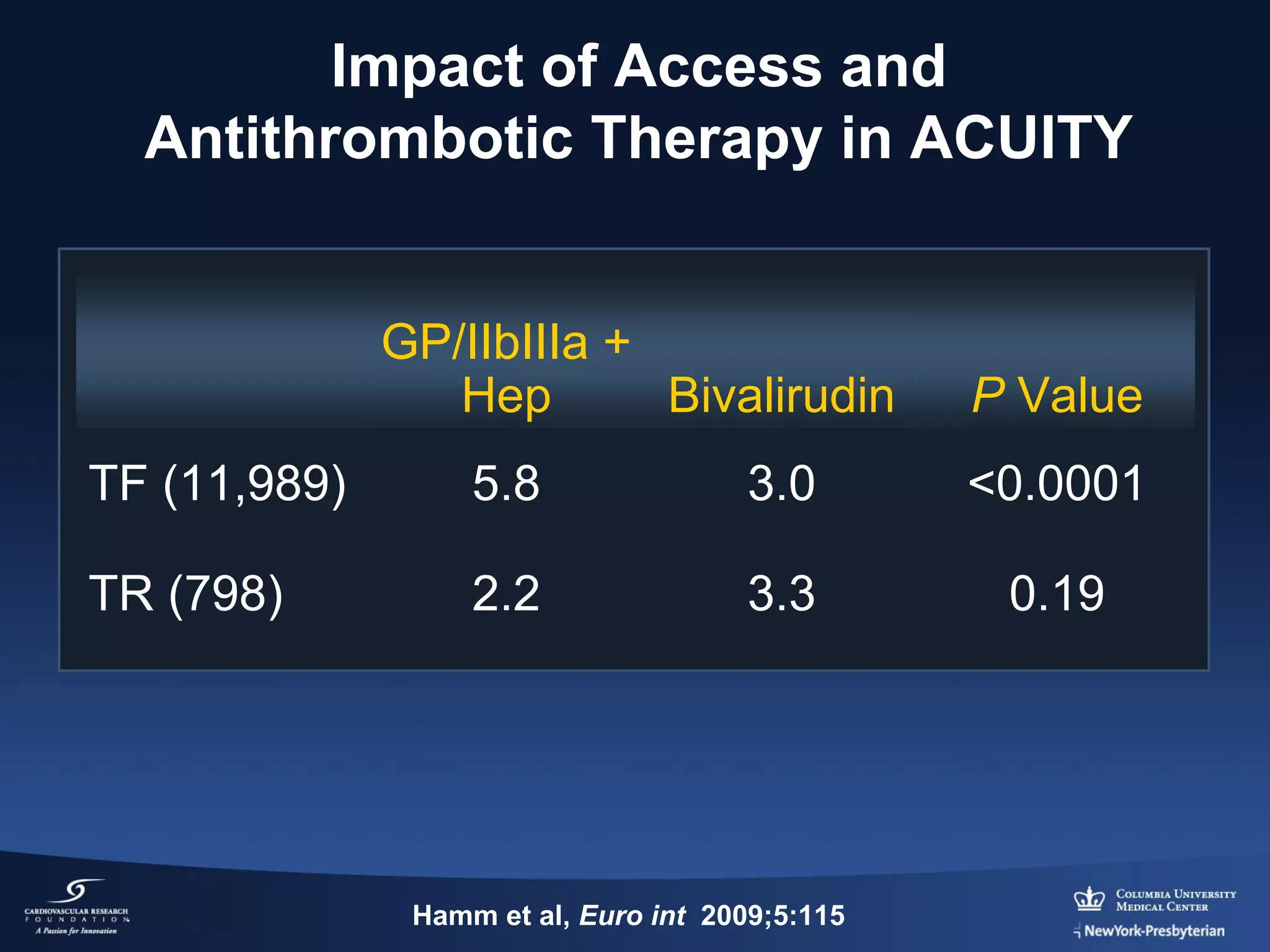

This document discusses the advantages and disadvantages of radial versus femoral artery access for percutaneous coronary intervention (PCI). Key findings from the RIVAL trial show that while radial access was associated with fewer major vascular complications compared to femoral, there was no significant difference in rates of death, heart attack, stroke or bleeding. However, radial access was linked to shorter procedure time, less bleeding, lower costs, fewer complications and greater patient satisfaction. The document concludes that while both approaches have merits, operators should become proficient in both to choose the most appropriate access site based on the patient's clinical situation and preferences.






















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












