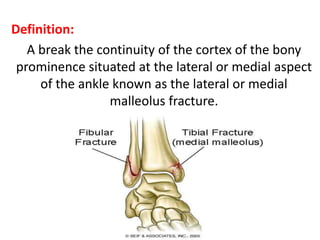
1) A malleolar fracture is a break in the bony prominence on the lateral or medial side of the ankle.
2) The majority are unimalleolar or bimalleolar fractures, most commonly caused by a twisting injury of the ankle.
3) Classification systems like the Weber system categorize fractures based on their location and relationship to the ankle joint. Displaced or unstable fractures often require open reduction and internal fixation to heal properly.
































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



