Downloaded 10 times
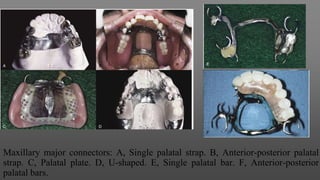
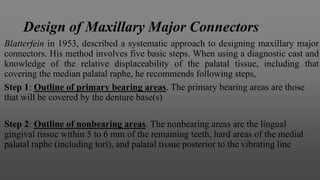
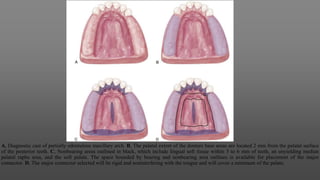

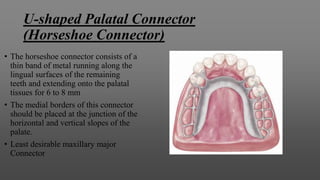
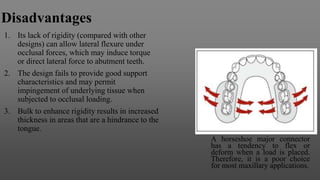
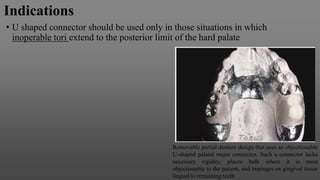
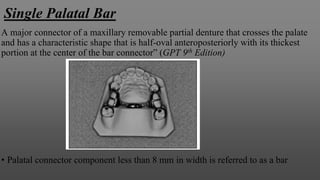
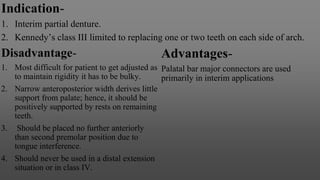
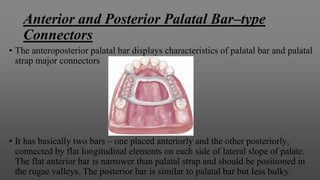

Maxillary major connectors are an important component of removable partial dentures that join the denture bases on each side of the dental arch. There are several types of maxillary major connectors including single palatal straps, combination anterior and posterior palatal straps, palatal plates, U-shaped connectors, single palatal bars, and anterior-posterior palatal bars. The ideal major connector is rigid, protects soft tissues, provides indirect retention, promotes patient comfort, and is self-cleansing. Proper design of the major connector involves outlining the denture base areas, non-bearing tissues, and connector areas on the diagnostic cast.
























![Differences-Between-Cast-Restoration-and-Amalgam[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/411598117-differences-between-cast-restoration-and-amalgam1-240425113051-8a78e12c-thumbnail.jpg?width=640&height=640&fit=bounds)










































