Download as PDF, PPTX





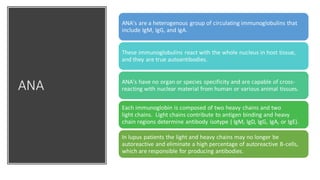
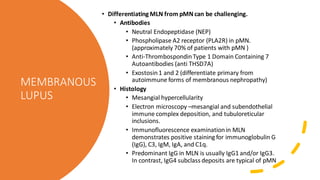
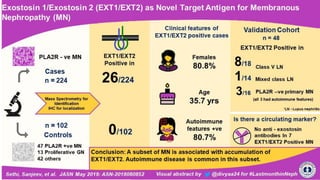

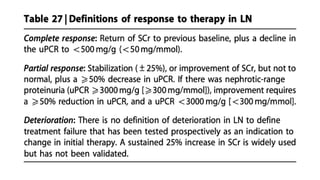
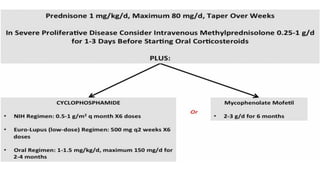
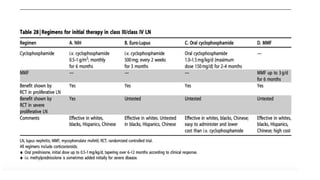

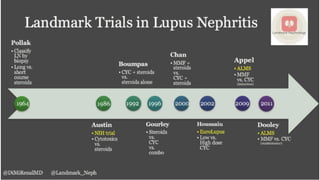


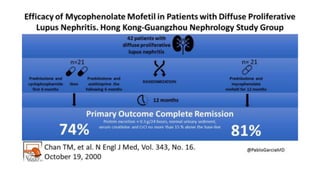
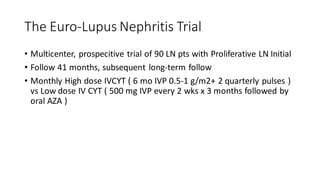
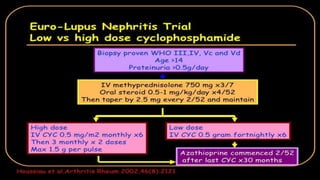
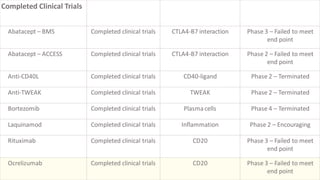
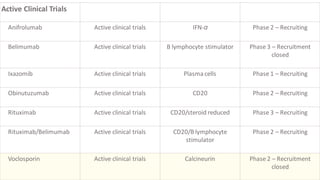
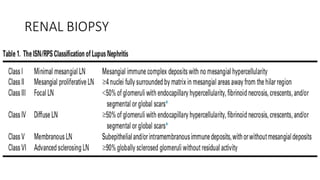
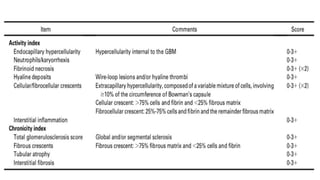
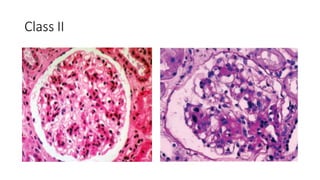
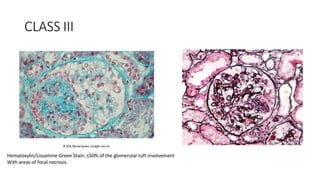
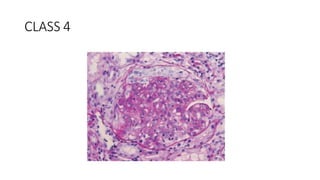

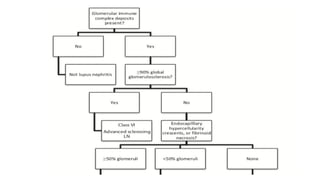


The document discusses the pathogenesis of lupus nephritis, including the loss of immune tolerance leading to autovaccination and persistent antinuclear antibodies, with a subset of patients developing lupus nephritis depending on additional genetic susceptibility factors; it also covers the classification, treatment approaches including immunosuppressive therapies, and clinical trials of lupus nephritis.



































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







