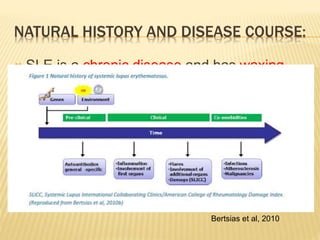
This document discusses systemic lupus erythematosus (SLE) and conditions that can mimic its presentation. It describes how SLE often has a waxing and waning chronic course that can vary in severity. Several infectious, inflammatory, and neoplastic conditions can present similarly to SLE through involvement of multiple organ systems and production of autoantibodies. Correct diagnosis requires a thorough history, physical exam, targeted testing, and biopsies to distinguish SLE from its mimickers. Serological similarities alone do not confirm SLE if clinical features are inconsistent.










































![REFERENCE:
1. Biro E, Bako G, et al. Association of systemic and thyroid autoimmune diseases. Clin Rheumatol.
2006; 25:240.
2. Meyer O. Parvovirus B19 and autoimmune diseases. Joint Bone Spine.2003;70:6.
3. Borreliosis mimicking lupus-like syndrome during infliximab treatment. Molin S, Ruzicka T, Prinz JC.
Clin Exp Dermatol. 2010 Aug;35(6):631-3. Epub 2010 Feb 20.
4. Immunological features of visceral leishmaniasis may mimic systemic lupus erythematosus. Sakkas
LI, Boulbou M, Kyriakou D, Makri I, Sinani C, Germenis A, Stathakis N. Clin Biochem. 2008 Jan;41(1-
2):65-8. Epub 2007 Oct 25.
5. Systemic lupus erythematosus: an occasional misdiagnosis. Collins. DA, Bourke .BE. Annals of the
Rheumatic Diseases 1996; 55: 421-422.
6. Allen IV, Miller JHD, Shillington RKA: Systemic lupus erythematosus clinically resembling multiple
sclerosis and with unusual pathological ultrastructural features. J Neurol Neurosurg Psychiatry
42:392, 1979. [PMID: 221619]
7. Lela A Lee. Lupus Erythematosus. Bolognia: Dermatology. (2nd ed.)ISBN: 9781416029991.
8. Orteuu CH, Buchanan JAG, Hutchison I, et al: Systemic lupus erythematosus presenting with oral
mucosal lesions: easily missed. Br J Dermatol 2001; 144:1219-1223
9. . Al-Hashimi H, Bhowmik A. Generalised lymphadenopathy as the first manifestation of lupus
nephritis. BMJ Case Rep. Published online: 22 Apr 2010. doi:10.1136/ bcr.08.2009.2221.
10. Edworthy SM. Clinical manifestations of systemic lupus erythematosus. In: Harris ED, Budd RC,
Firestein GS, et al. eds. Kelley’s textbook of rheumatology. 7th edn. Philadelphia, PA: WB Saunders,
2005:1201–24.
11. Horta-Baas G, Hernández-Cabrera MF, Barile-Fabris LA, Romero- Figueroa Mdel S, Arenas-Guzmán
R. Multibacillary leprosy mimicking systemic lupus erythematosus: case report and literature review.
Lupus. 2015;24(10):1095–102.](https://image.slidesharecdn.com/lupusmimicker2-230209090204-868a18a5/85/Lupus-mimicker2-pptx-47-320.jpg)
























































































