OBJECTIVES
• Overview ofthe relevant thoracic anatomy
• Imaging modalities and oncologic applications in Lung
and Esophageal Cancer.
5.
TRACHEOBRONCHIAL TREE
• Trachea
–begins at lower border of
cricoid cartilage at C6 level
– T 5 level, T 4 on
inspiration and T 6 on
expiration)
– Extends to carina at sternal
angle at T5 level
6.
Main bronchi
• Carinais the point of tracheal bifurcation
• Lies at T5(T4 in expiration, T6 at inspiration)
• Carinal angle
– 60°(20° right & 40° left)
– larger in children; increases by 10-15* in recumbency
– Marker of atrial enlargement if widened on PA CXR
• Right main bronchus is shorter wider and more vertical than
the left
• The left main bronchus is longer, more horizontal and
narrower
9.
PA (1)trachea (2)right mainstem bronchus (3) left mainstem bronchus (4)aortic knob/arch(5)
azygos vein emptying into superior vena cava right interlobar pulmonary artery (6), (7), left
pulmonary artery(8)right upper lobe pulmonary artery (truncus anterior) (9) right inferior pulmonary
vein (10) right atrium (11)left ventricle
Lateral(1), pulmonary outflow tract (2), (3), ascending aorta aortic arch (4), brachiocephalic vessels
(5), trachea (6), right upper lobe bronchus (7), left upper lobe bronchus (8), right pulmonary
artery(9), left pulmonary artery(10), confluence of pulmonary veins
Review of Xray Anatomy
10.
tttt
Acinus
The functional unitfor gas exchange distal to the
terminal (lobular) bronchioles. The acini are formed by
the bronchioli respiratorii, the ductuli alveolares, the
alveoli, and the local pulmonary vessels
1
0
Bronchopulmonary segments
• Thisis the cone-shaped
smallest, functionally
independent region of a
lung.
– Supplied by a segmental
bronchus and a pulmonary
artery branch.
– Pulmonary vein trib. pass
on the margins of
segments.
• 10 on the right and eight
on the left
12
13.
The Secondary Lobule
•It is the smallest lung unit that is
surrounded by connective tissue septa.
• It measures about 1-2 cm and is made
up of 5-15 pulmonary acini, that contain
the alveoli for gas exchange.
• Is key to HRCT terminology because
Interpretation of interstitial lung diseases is
based on the type of involvement of the
secondary lobule.
13
14.
Secondary lobule ctd.
•Terminal bronchiole in the
center, paralleled by the
centrilobular artery.
• Septal periphery of the lobule-
Pulmonary veins and
lymphatics
• Usually only a few seen
14
15.
SECONDARY LOBULE ctd...
•Centrilobular area…(in blue)
• site of the airways diseases
e.g respiratory bronchiolitis, emphysema
• Perilymphatic area…(in yellow)
• site of lymphatics dzs of the interlobular septa
e.g sarcoid, lymphangitic carcinomatosis,
pulmonary edema).
15
16.
Pulmonary vessels
• Pulmonaryarteries
– Arise from pulm trunk
– Rt and left
• Pulm veins
– 2per side(superior and inferior)
– Begin at hilum, empty into left atrium
• Bronchial aa/veins
– Nutritive function to lung
• Innervation
– vagus nn: constricts bronchioles
– sympathetic chain: dilates
17.
Lymphatic drainage
• Twolymphatic systems:
– central network, along the bronchovascular bundle
(centrilobular area)
– peripheral network in interlobular septa and along
the pleural linings(perilymphtic area)
• These drain to the hila bronchopulmonary
nodes→ tracheobronchial nodes & paratracheal
nodes→bronchomediastinal trunks
17
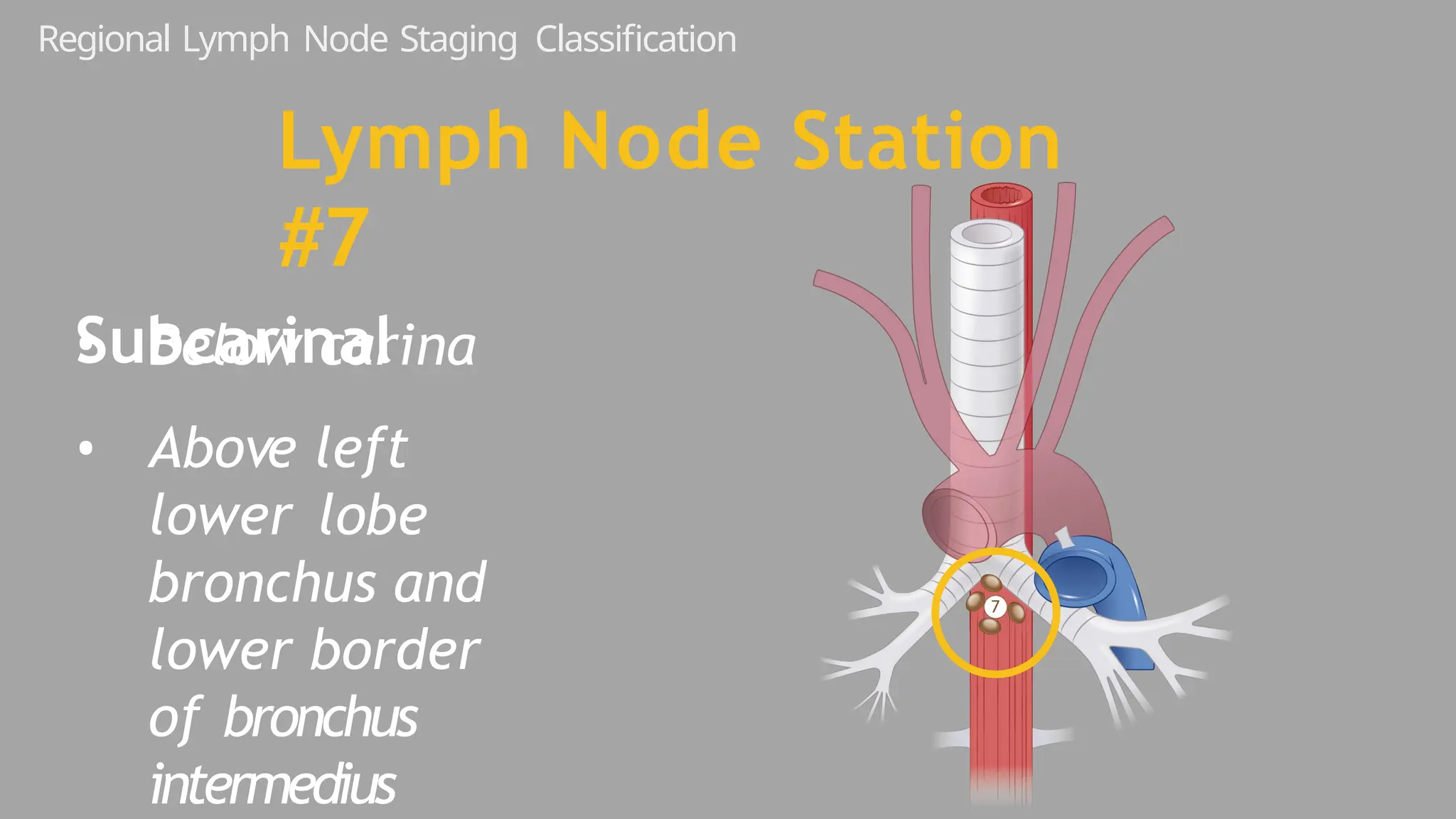
Regional Lymph NodeStaging Classification
Lymph Node Station
#2
2R: right
upper
paratracheal
24.
Regional Lymph NodeStaging Classification
Lymph Node Station #3a
Pre-vascular
• Below apex
• Above carina
• Posterior to sternum
• Anterior to SVC
and left common
carotid artery
25.
Regional Lymph NodeStaging Classification
Lymph Node Station #3a
Pre-vascular
Regional Lymph NodeStaging Classification
Lymph Node Station #3p
Retrotracheal
28.
Regional Lymph NodeStaging Classification
Lymph Node Station #4R
4R: right lower
paratracheal and
pretracheal
• Below innominate vein
• Above azygous vein
• Extends to left
lateral border of
trachea
29.
Regional Lymph NodeStaging Classification
Lymph Node Station #4R
4R: right lower
paratracheal and
pretracheal
30.
Regional Lymph NodeStaging Classification
Lymph Node Station #4L
4L: left
lower
paratracheal
• Medial to
ligamentum
arteriosum
• Below upper
margin of aortic
31.
Regional Lymph NodeStaging Classification
Lymph Node Station #4L
4L: left
lower
paratracheal
32.
Regional Lymph NodeStaging Classification
Lymph Node Station #4L
4L: left
lower
paratracheal
• Medial to
ligamentum
arteriosum
33.
• Lateral to
ligamentum
arteriosum
•Below bottom of aortic
arch
• Above top of left MPA
Regional Lymph Node Staging Classification
Lymph Node Station
#5
Subaortic (aorto-
pulmonary window)
34.
Regional Lymph NodeStaging Classification
Lymph Node Station
#5
Subaortic (aorto-
pulmonary window)
• Lateral to
ligamentum
arteriosum
35.
• Anterior andlateral
to ascending aorta
and arch
• Below top of aortic
arch
• Above bottom of arch
Regional Lymph Node Staging Classification
Lymph Node Station
#6
Para-aortic
Regional Lymph NodeStaging Classification
• Below azygous
vein on right
• Below top of left
pulm artery on
left
• Above interlobar
region bilaterally
Lymph Node Station #10
Hilar
SPECIAL DIAGNOSTIC PROCEDURES
•PERCUTANEOUS FINE NEEDLE ASPIRATION
• CT guided
• Excellent for peripheral nodules
• limitation is that it cannot rule out malignancy
• BRONCHOSCOPY
• Able to visualize tracheobronchial tree upto 2nd /3rd segment
• Cytologic brushing/biopsy forceps are used to acquire specimens
50
51.
• ENDOSCOPIC ULTRASOUND
•Evaluation of mediastinal /hilar lymph nodes
• ENDOBRONCHIAL U/S GUIDED NEEDLE TRANSBRONCHIAAL
ASPIRATION
• Involves FNA sampling at levels 2,4,7,10
• 98% sensitivity 92% specificity
• THORACOCENTESIS
• Evaluation of pleural effusion
• Can be used simultaneously with thoracoscopy to evaluate the pleural space
further
51
52.
• MEDIASTINOSCOPY
• Mostaccurate technique to assess lymph node stations 2,4,3,7
• Has been replaced with U/S
• Considered when less invasive techniques are non diagnostic
• Recommended to rule out N3 disease/identify N2 disease for induction chemotherapy
• THORACOSCOPY
• Video assisted
• Used for diagnosis, staging and resection
• Valuable in evaluating pleural disease
• Useful in evaluating mediastinal nodes inaccessible by standard mediastinoscopy/U/S
52
53.
LUNG CANCER
• Lungcancer is a heterogenous (not one disease) , with multiple histologic subtypes
and molecular phenotypes
• Staging of Lung cancer offers both theraupetic and prognostic guidance, imaging aids
in determining anatomic extent of disease
• Proper initial evaluation and and staging of patients is important for appropriate
theraupetic decision making.
• CT is an imortant component in staging, FDG PET used to assess Nodal and
extrathoracic metastasis
54.
WHO Classification ofLung Cancer
• Non-small cell lung cancer (NSCLC)- Most common 85%
➢ Adenocarcinoma (40%)– Ass with smoking, most common in non smokers.
Multiple histologic subtypes, including acinar, papillary, solid, micropapillary, or
lepidic. Peripheral, solitary pulmonary nodule with irregular or spiculated
margins, cavitation is rare
➢ Squamous cell (30%)- Highly smoking related, occur as central endobronchial
mass, affect proximal bronchi-causes obstruction cough, haemoptysis and
post obstructive pneumonia, most likely to cavitate
➢ Large cell (15%)- peripheral, poorly maginated
➢Carcinoid-
• Small Cell Carcinoma (15%)- decreasing incidence, always in smokers, Small
Central mass with mediastinal LNs, rapid growth and spread, paraneoplastic
syndromes
54
56.
ROUTES OF SPREAD
Localextension
• Direct extension from tumor to surrounding tissues
• Most commonly involves
• Pleural extension- Most frequently results in pleural metastases in caudal and posterior parts of pleural spaces
• Chest wall
• Esophagus
Lymphatic spread
• Through lymphatic system to neighboring or distant lymph nodes
• Lymphangitic spread can be associated with hematogenous dissemination, Followed by invasion of adjacent interstitium and lymphatics
esp in adenocarcinomas (lymphangitic carcinomatosis)
• Subsequent tumor spread toward hilum or lung periphery
Distant metastases
• When tumor develops invasive behavior, it has access to rich pulmonary capillary networks
• Pulmonary veins are common route of metastasis, hematogenous spread is high with adenocarcinomas, occurs late in SCC
• Adrenals, liver, brain, bones
• Disemmination and tumor emboli are common and are a prognostic factor for overall survival
57.
Staging Work-Up
•Complete H&P, CBC, Chemistry panel
•CXR-limited role now
•CT chest & upper abdomen with contrast
•PET CT to evaluate LNs and distant metastasis
•CT scan Brain/MRI- Stage III and IV
•Pulmonary function tests for Surgical Candidates
•Thoracocentesis with cytology in patients with Pleural Effusion
58.
DIAGNOSTIC IMAGING MODALITIES
CHESTRADIOGRAPH
• Can be used to evaluate a patient presenting with chest symptoms with documented sensitivity of 77-80 %
CLINICAL UTILITY
• Systematic review of all chest anatomic compartments
• Lungs and airways
• Nodule, mass-Airway-related nodule/mass
• Atelectasis, consolidation
• Hilar
• Enlargement from lymphadenopathy or mass
• Mediastinum- Focal mass or diffuse mediastinal enlargement
• Pleura
• Malignant pleural effusion ± pleural nodules/masses/thickening
• Chest wall
• Nodule, mass, infiltrative lesion
58
59.
• There isa large area of
airspace opacification in the
left mid-lower zone.
• There is silhouetting of the left
heart border on the frontal
projection, placing the
abnormality in the lingula
segments of the left upper
lobe.
• The oblique fissure appears
lobulated.
• The right lung and pleural
recesses appear clear.
60.
CHEST COMPUTED TOMOGRAPHY
•Recommended for all patients
suspected of lung cancer
• CT CHEST with contrast
extending to include the liver
and the adrenal glands
• CT is able to establish: T stage,
presence of atelactesis,
invasion of adjacent
structures and proximal
extent of tumor
61.
CT CHEST…
Contrast EnhancedCT is used to stage most patients
○ Tumour (T) staging
– Size and location
– Extent of disease
□ Relationship to airways and vessels
□ Invasion of adjacent structures
□ Tumour nodules
– PS: CT is Inferior to MR in detection of locoregional invasion of chest wall, mediastinum, and
diaphragm
62.
• LYMPH NODE(N) STAGING
• Anatomic criteria used on CT
• Lymph node size not always reliable
• Inferior to PET/CT for detecting lymph node metastases
• METASTASIS (M) STAGING
• PET/CT-Superior to CT in detecting metastases
• RESTAGING
• CECT routinely used for assessment of treatment response, surveillance, and restaging – Inferior to PET/CT in many studies
63.
NSCLC Staging
• Oncethe histologic diagnosis of NSCLC has been established, the extent of disease must be determined. The
stage of disease will dictate therapy.
• All patients must undergo a complete history and physical examination, chest x-ray, CT scan of the chest and
upper abdomen (to include the adrenal glands), a complete blood count, and blood chemistry tests that include
electrolyte and liver enzyme studies
• All patients with stage II to IV disease should have evaluation of the brain, with magnetic resonance imaging
(MRI) if possible.
• For stage I to III NSCLC, 18Ffluorodeoxyglucose (FDG)-PET should be performed to evaluate mediastinal nodes
and for distant metastases.
67.
T1
• ≤ 3cm in greatest
dimension
• Surrounded by lung
or visceral pleura
• Not in main bronchus
•Is a standardin staging, limited use due to cost
•Purpose:
1. stage primary tumor characteristics
2. distinguish atelectasis from tumor
3. identify nodal metastasis
4. identify distant metastasis
•Able to detect 0.5cm tumor
90
PET CT SCAN
91.
PET CT SCANctd…
Staging
• More accurate than CT in delineating extent of tumor involvement
• Accuracy: CT: 68%; PET: 46%; PET/CT: 86%; visually corrected PET/CT: 72%
• PET and PET/CT improve detection of lymph node metastases
• Accuracy: 75-80%; sensitivity: 70-75%; specificity: 90-95%
• Superior to CT and PET alone
• Metastases
• Superior to CT and PET for pericardial metastases
• More sensitive and accurate than bone scan (91% and 94% vs. 75% and 85%, respectively)
• Low sensitivity for brain metastases due to increased FDG uptake of brain parenchyma
• Monitoring, surveillance, and restaging
• Not recommended for routine follow-up
• Often performed for concerning symptoms or suspicious findings on CT
91
92.
PET-CT is recommendedin : NCCN
(a) Diagnosis in patients with one or two pulmonary nodules
(b) Initial staging except if multiple distant metastases exist
(c) Restaging stage III or IV after 2–3 months after treatment or before surgery
(d) Restaging in patients with symptoms suggestive of recurrence
(e) Radiation therapy
92
93.
SCLC
• Imaging isprincipal method of staging SCLC
• Chest CT with i.v. contrast, incl. adrenals
• Brain imaging, MR preferable to CT
• FDG-PET often obtained
• Abdomen CT and Tc-99m bone scan if PET not available
94.
SCLC: Staging Criteria
-According to Veterans Administration Lung Cancer Group (VALG)
Limited Stage 1/3
Confined to one hemithorax and regional lymph nodes
Unlike NSCLC, mets to ipsilateral & contralateral supraclav, mediastinal LNs are considerred limited
disease
Extensive stage 2/3
Positive pleural effusion, contralateral lung nodules, contralateral supraclavicular LNs, distant
metastasis
Asymptomatic metastasis -70% at diagnosis
95.
Small Cell LungCancer
90-95% of SCLC arise from lobar or main bronchi thus most commonly manifest as a large mass centrally
located within the parenchyma or a mediastinal mass involving at least one hilum (paratracheal node pointed)
Lung nodule with mediastinal adenopathy;
limited-stage disease
98.
Small Cell LungCancer (SCLC)
Primary Tumor
• 90 - 95% are centrally located
(hilar/mediastinal), arising from main bronchi
• Often a hilar/mediastinal mass without a visible
lung nodule
• Usually large and bulky
• Often surrounds and narrows central bronchi
• May have post-obstructive atelectasis / pneumonia
Small Cell LungCancer (SCLC)
Common Sites of
“Extensive Stage” Spread
• Bone (19-38% of cases)
• Liver (17-34% of cases)
• Adrenals (10-17%)
• Brain (up to 14%)
Small Cell LungCancer (SCLC)
FDG-PET
• PET ~ 95% accurate in detecting
extensive disease, affects choice of
therapy
• PET may change management in ¼ of
patients
• Upstaging more common than downstaging
• Commonly modifies determination of
Small Cell LungCancer (SCLC)
Brain Imaging
• Brain metastases in 10-15% of neurologically
asymptomatic patients
• Including 12% of patients otherwise thought to
have limited stage disease
• Head MR and CT more sensitive than PET
• MR more sensitive and specific compared to CT
SUBTYPES
• squamous cellcarcinoma of oesophagus: 81-95% (worldwide)
• adenocarcinoma of oesophagus: 4-19% (worldwide)
➢ arising from mucosal/submucosal glands, heterotopic gastric mucosa, or columnar-lined epithelium
➢ >90% related to Barrett oesophagus
➢ tend to occur at the gastro-oesophageal junction
other types
• mucoepidermoid carcinoma
• adenoid cystic carcinoma (ACC)
• spindle-cell squamous carcinoma
• leiomyosarcoma
• rhabdomyosarcoma
• fibrosarcoma
• lymphoma
11
8
121.
CHEST RADIOGRAPH
• Manyindirect signs can be sought on a chest radiograph and these include:
• widened azygo-oesophageal recess with convexity toward right lung (in 30% of distal
and mid-oesophageal cancers)
• thickening of posterior tracheal stripe and right paratracheal stripe >4 mm (if tumour
located in the upper third of oesophagus)
• tracheal deviation or posterior tracheal indentation/mass
• retrocardiac or posterior mediastinal mass
• oesophageal air-fluid level
• lobulated mass extending into gastric bubble (Kirklin sign)
• repeated aspiration pneumonia (with tracheo-oesophageal fistula)
12
1
122.
FLUOROSCOPY/ESOPHAGOGRAM
• Contrast/ bariumswallow
• irregular stricture
• prestricture dilatation with 'hold up'
• shouldering of the stricture
• Although useful in evaluating
length and severity of malignant
strictures, which can be used in
treatment planning, it does not
provide useful staging information
12
2
123.
ENDOSCOPIC ULTRASOUND
• Themost accurate imaging modality for the T staging of oesophageal cancer. It defines
the layers of the oesophageal wall hence can differentiate T1, T2, and T3 tumours.
• The oesophagus consists of five layers:
1.first hyperechoic layer represents the interface between the balloon and the superficial
mucosa
2.second hypoechoic layer represents the lamina propria and muscularis mucosae
3.third hyperechoic layer represents the submucosa
4.fourth hypoechoic layer represents the muscularis propria
5.fifth layer represents the interface between the adventitia and surrounding tissues
12
3
124.
ENDOSCOPIC ULTRASOUND
The mostaccurate imaging modality for the T
staging of oesophageal cancer. It defines the
layers of the oesophageal wall hence can
differentiate T1, T2, and T3 tumours.
The oesophagus consists of five layers:
1.first hyperechoic layer represents the interface
between the balloon and the superficial mucosa
2.second hypoechoic layer represents the lamina
propria and muscularis mucosae
3.third hyperechoic layer represents the
submucosa
4.fourth hypoechoic layer represents the
muscularis propria
5.fifth layer represents the interface between the
adventitia and surrounding tissues
12
4
125.
Contrast Enhanced CT(CECT)
• Determination of T4 disease is most important role of CT in evaluating local disease: Tracheobronchial, aortic, or pericardial involvement
• Unable to adequately differentiate between T1, T2, and T3 disease
• Limited in determining depth of esophageal wall invasion
• Better performance for higher stage lesions (T3,T4)
Aortic invasion is suggested by
• □ ≥ 90° of aorta in contact with tumor
CT criteria for local invasion include
• □ Obliteration of triangular fat space between esophagus, aorta, and spine adjacent to primary tumor
Tracheobronchial invasion is suggested by
• Displacement of trachea or bronchus
• Indentation of tracheal or bronchial posterior wall by tumor
• Tracheobronchial fistula or tumor extension into airway lumen is definite sign of tracheobronchial invasion
Pericardial invasion is suspected if there is
• Pericardial thickening
• Pericardial effusionith limited diagnostic accuracy in lower stage lesions (T1, T2)
12
5
126.
CECT
• CT haspoor sensitivity for depiction superficial lesions
• Irregular, thick, enhancing esophageal wall, resulting in proximal esophageal dilatation
• Normal distended esophageal wall is usually < 3 mm thick
• Any wall thickness > 5 mm is considered abnormal
• Wall thickening is usually asymmetric, causing eccentric luminal narrowing
• Less accurate than EUS and biopsy
• Determining involvement of nodes depends on nodal size
• Intrathoracic and abdominal lymph nodes > 1 cm in diameter
• Supraclavicular lymph nodes with short axis > 5 mm
• Retrocrural lymph nodes with short axis > 6 mm
• Portocaval lymph node, which has big longitudinal axis
• Limitations
• Micrometastasis may be found in normal-sized nodes
• Some enlarged nodes may be reactive
• Cannot detect peritumoral /conglomerate lymph
• nodes that are inseparable from tumor
12
6
127.
T: D epthof
Invasion
Inability of CT to determine degree of extension
within esophageal wall (T1-T3 disease)
128.
Y
CT may allowfor exclusion of T4
disease (invasion of adjacent
structures) via the presence of
T: D epth of
Invasion
129.
T: D epthof Invasion
CT findings suggestive of T4 disease:
• Loss of intervening fat plane
• D isplacement of mediastinal structures
• > 90 degree contact of tumor with aorta
• Pericardial thickening or effusion
• Variable sensitivities and specificities reported
in the literature for these findings
130.
CT Imaging ofEsophageal Cancer
Aortic invasion and aorto-esophageal
131.
T: D epthof
Invasion
Tracheal invasion with tracheoesophageal
132.
N: Regional Nodal Involvement
CT assessment for nodal metastases
• Sensitivity 42-50%
• Specificity 83-93%
Sensitivity limited as normal sized lymph
nodes (< 1cm short axis) may have
metastatic disease
133.
CT Imaging ofEsophageal Cancer
Enlarged gastro-hepatic lymph
N: Regional N odal
Involvement
CT Imaging ofEsophageal Cancer Y
Metastatic disease to the
137.
Limits of CT
•Not for primary diagnosis
• Suboptimal evaluation for the
degree of esophageal wall invasion
• Detection of regional lymph
node involvement limited
138.
PET CT SCAN
•FDG PET-CT is useful for detecting oesophageal primary tumors yet it has little role in helping
determine the specific T classification because it provides limited information about the depth of
tumor invasion.
• PET-CT is also superior to CT for detecting lymph node metastases and can depict metastases in
normal-sized lymph nodes through the uptake of FDG.
• PET-CT has a primary role in the depiction of distant sites of metastatic disease.
• The most common sites of distant metastases detected at PET (but frequently missed at CT) are
the bones and liver.
• Higher sensitivity than CT in detection of primary esophageal cancer, as most esophageal
malignancies are FDG avid
• Helpful in detection of esophageal tumors in patients with metastases of unknown origin
• False-negatives in small T1 and T2, necrotic or mucinous tumors
• False-positives due to esophagitis secondary to GERD, infectious esophagitis or after endoscopy
intervention
13
8
139.
r
Indications for PET/CT
•Strategy to detect distant metastases
• Improving specificity of lymph node staging
• Combining PET/CT and EUS-guided biopsy
as preoperative work-up for the highest nodal
yield
PET/CT of EsophagealCancer
Primary Tumor
• PET/CT has overall sensitivity 80% for
primary esophageal cancer
• Sensitivity is close to 100% for T3 and T4
tumors
• BUT, sensitivity is only 43% for T1 tumors
• PET/CT cannot detect in-situ and T1a tumors
• PET/CT cannot determine T stage
Pitfalls
• Mild esophagealuptake (SUVmax < 4.0) may relate
to esophagitis or lower esophageal sphincter
• Hiatal hernias, benign stricture after dilatation, post-biopsy
and esophageal leiomyomas can have mild FDG uptake
(false- positives)
• Small intracapsular nodal metastases have a high
false- negative rate
• Intense uptake in the primary tumor may obscure
subtle abnormal adjacent nodes
• Synchronous primary neoplasms in 5.5-8% of patients
148.
RESTAGING
• PET/CT –Most sensitive method of differentiating chemotherapy responders from no responders
• Responders demonstrates decrease in maximum standardized uptake value (SUVmax) of 45-60% between baseline
and post chemotherapy staging
• No responders might demonstrate persistent FDG uptake in tumor, which correlates with persistent viable macroscopic
malignancy and poor clinical outcome
• Added value in differentiating tumor recurrence from posttreatment changes
• Posttreatment changes may include fibrosis and inflammation, making CT appearance nonspecific
• Inflammation related to post endoscopy biopsy or stent placement or chemoradiation-induced esophagitis or ulceration
might mimic viable tumor
• Perform no sooner than 3-4 weeks after completion of chemoradiation
14
8
149.
• Restaging importantafter neoadjuvant chemotherapy to determine if patient is surgical candidate by
detecting new metastatic disease, which can occur in 17% of cases and can preclude surgery
• May identify complications of therapy
➢ Esophagitis
➢ Tracheoesophageal fistula
14
9
Editor's Notes
#5 Cervical
The anterior relations are as follows: • Anterior: isthmus of thyroid anterior to the second, third and fourth rings
inferior thyroid veins strap muscles: sternohyoid and sternothyroid • Posterior: oesophagus and recurrent laryngeal nerves • Lateral: lobes of thyroid gland common carotid artery
The thoracic relations are as follows: • Anterior: brachiocephalic and left common carotid arteries left brachiocephalic vein • Posterior: oesophagus and left recurrent laryngeal nerve • Left lateral: arch of the aorta left common carotid and left subclavian arteries • Right lateral: right brachiocephalic artery right vagus nerve arch of the azygos vein pleura (in direct contact unlike the other side)
#6 Right main bronchi relations
anterior: superior vena cava right pulmonary artery; posterior: azygos vein; and • superior: arch of azygos vein
The bronchus to the upper lobe arises almost immediately after the tracheal bifurcation, entering the hilum of the lung separately
The relations of the left main bronchus are as follows: • anterior: pulmonary trunk; • posterior: oesophagus descending aorta; and superior: aortic arch; pulmonary artery
#7 segmental bronchi each named after its supplying lobe segments
#10 has a diameter of 7.5 to 8.5 mm and contains 3000 to 4000 alveoli. The whole lung consists of 15,000 to 20,000 acini.
#11 Major fissureT 4 /T 5 posteriorly to the diaphragm anteroinferiorly The left major fi ssure is more vertically orientated than the right.
Minor fissure runs horizontally from the hilum to the anterior and lateral surfaces of the right lung at the level of the fourth costal car- tilage Its posterior limit is the right oblique fi ssure, which it meets at the level of the sixth rib in the midaxillary line It is anatomically complete in only one-third of subjects and is absent in 10%
#60 The CT shows a tumor mass , which is obstructing the right upper lobe bronchus and it is extending into the distal right mainstem bronchus. There is post-obstructive consolidation of the entire right upper lobe.
#68 T1 lesions. small cancers, no more than three centimeters in greatest dimension, surrounded by lung, or surrounded by visceral pleura. These cancers do not involve a main bronchus. T1 is broken down depending on size
#69 There's a new category called T1a(mi). These are the minimally invasive, early bronchogenic adenocarcinomas. They are solitary and they show a predominantly lepidic pattern under the microscope and there's no more than five millimeters of stromal invasion in greatest dimension. This is a histologic category, but we do see a correlate on our CT scans. Generally, these lesions show up as small subsolid nodules, like this one, that are mostly ground glass but they have a small central solid component. It is the solid component that corresponds to the area of invasions, so the solid component should be no more than five millimeters in diameter.
#72 The T2 category also includes invasion of the visceral pleura and that is suggested in this patient with a left upper lobe cancer that shows broad contact with the pleural surface.
#73 The T2 category also includes invasion of the visceral pleura and that is suggested in this patient with a left upper lobe cancer that shows broad contact with the pleural surface.
#74 T2 is also broken down by size. The T2a lesions are from 3-4 centimeters in diameter, and the T2b lesions from 4-5 centimeters in diameter.
#75 T3 category, these are larger cancers from 5-7 centimeters in greatest dimension. The T3 category includes chest wall invasion. On CT scanning, we look for frank rib destruction
#76 T3 also includes superior sulcus invasion as illustrated in this patient on an MR scan. We see a tumor here at the apex of the lung, it's growing out of the lung into the adjacent soft tissues here on a sagittal MR image and here on a coronal MR. MR is the modality of choice in diagnosing superior sulcus invasion and that would again constitute T3 disease. MR is also the modality of choice in looking for associated brachial plexus involvement by these types of tumors.
#79 T3 category- separate tumor nodules in the same lobe of the lung. There is severe underlying smoking-related emphysema and there are two nodules, both of these were cancers so this constitutes T3 disease, both on the same lobe of the lung.
#80 T4 category- these are the very large cancers more than seven centimeters in greatest dimension. The T4 category includes invasion of all of the structures listed
#81 The patient has a right lower lobe cancer- it's indenting the liver with diaphragmatic invasion.
#82 Also on the T4 category is mediastinal invasion. Sometimes the invasion is gross as in this pt
#83 A) the tumor is invading directly into the main pulmonary trunk B) there is tumor invasion of mediastinal fat in addition the tumor is invading into the superior vena cava