Downloaded 43 times

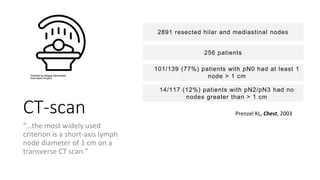
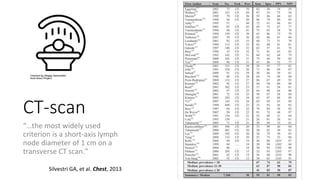
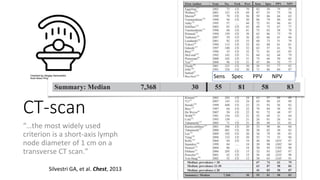
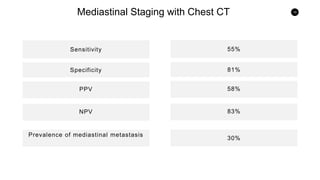

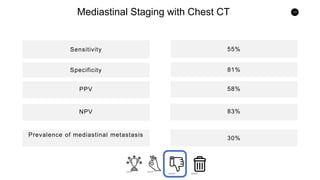
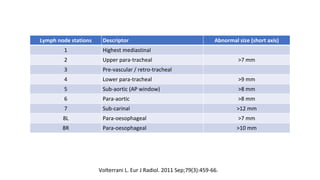
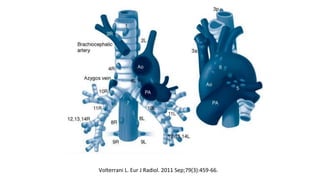
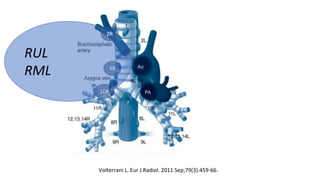
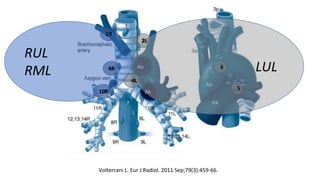

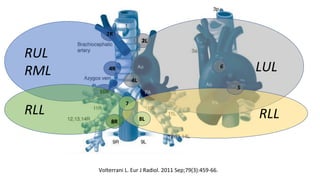
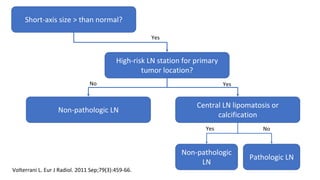
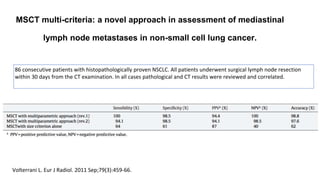
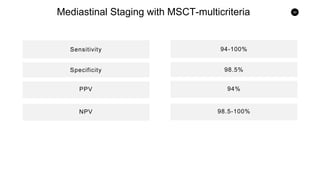
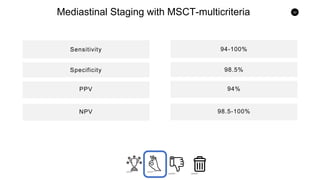
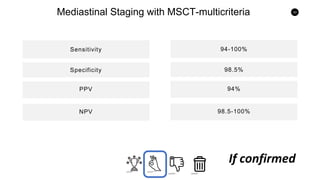
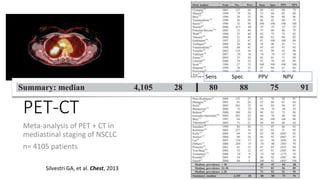
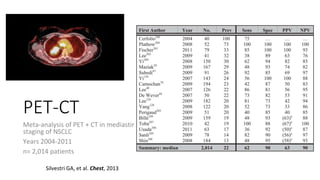
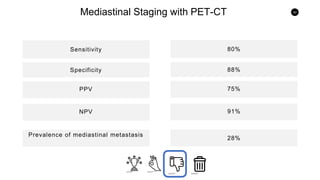
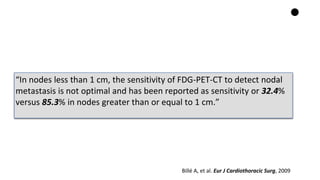
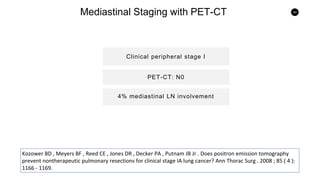
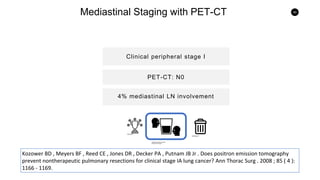
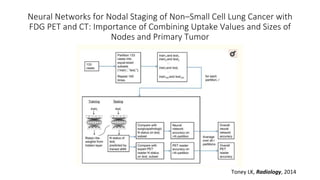
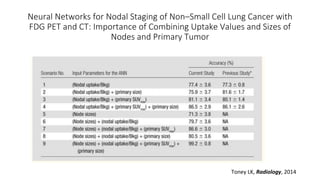
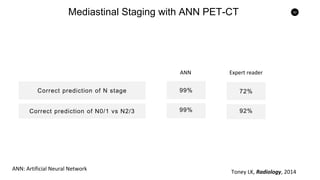
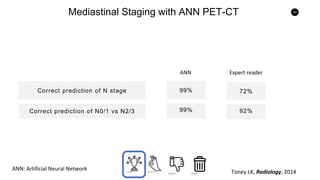
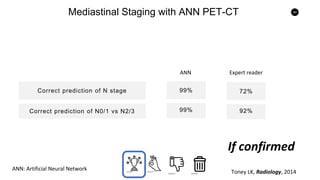
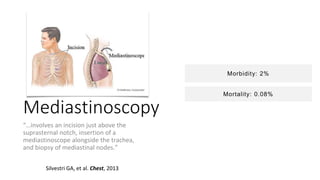
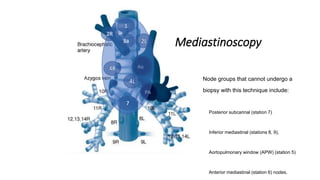
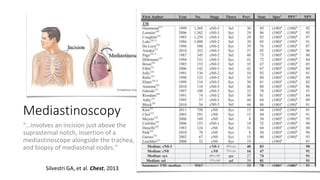
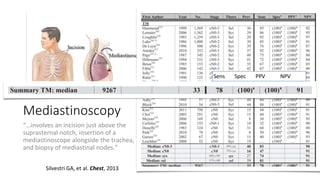

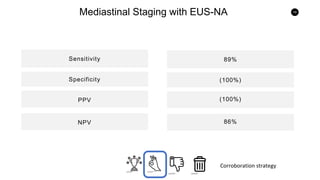
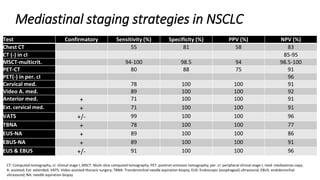
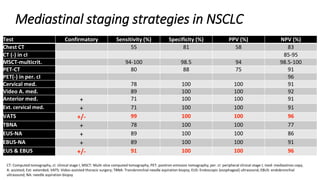

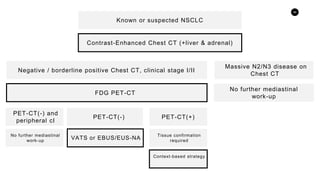


This document discusses mediastinal staging for non-small cell lung cancer (NSCLC). Chest CT has reasonable sensitivity (55%) and specificity (81%) for mediastinal staging but multi-station CT using lymph node size and location criteria can improve sensitivity to 94-100% and specificity to 98.5%. PET-CT further improves staging with a meta-analysis showing sensitivity of 80% and specificity of 88% but may miss metastases in small lymph nodes. Artificial neural networks analyzing PET-CT scans can predict mediastinal nodal stage with 99% accuracy. Tissue confirmation is still recommended when PET-CT indicates mediastinal involvement.