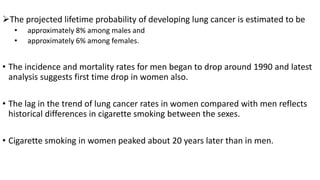
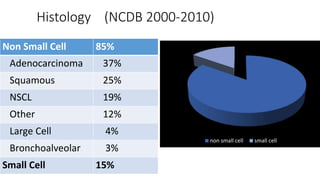
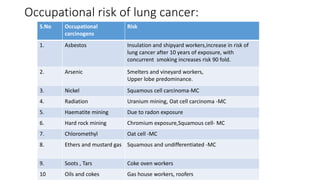
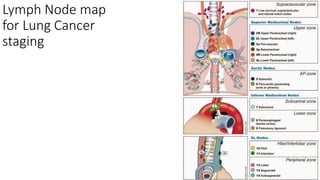
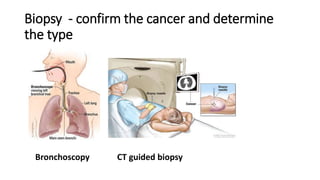
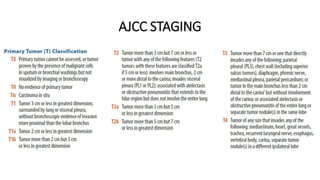
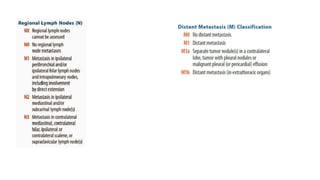
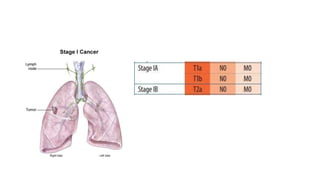
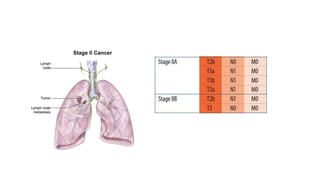
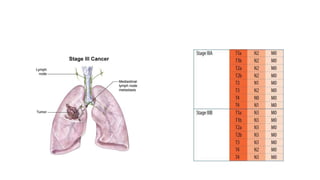
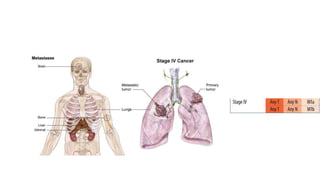
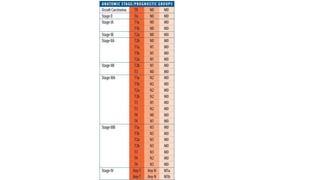
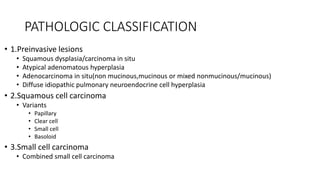
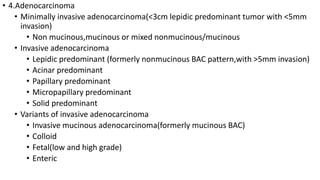
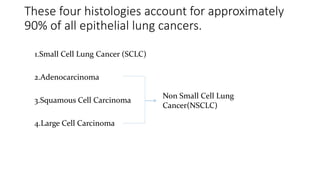
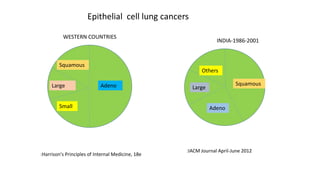
The document summarizes lung cancer anatomy, risk factors, epidemiology, clinical features, diagnosis, staging and pathological classification. It notes that tobacco consumption causes 80-90% of lung cancers. Diagnostic workup includes imaging like CT, PET scans and biopsies to determine cancer type which are most commonly adenocarcinoma, squamous cell carcinoma, small cell lung cancer or large cell carcinoma. Staging uses the AJCC TNM system and influences treatment options and prognosis.
![Parts of Lung
• Conical in shape
•
• Each lung has an apex,base,3 borders and 2 surfaces.
• Surfaces-
• Costal surface- broad and pressed against the rib cage.
• Mediastinal surface- smaller, concave and faces medially.
• Apex[apex pulmonis]-rounded & extends to the root of the neck[2.5-4cm above
the level of sternal end of first rib]](https://image.slidesharecdn.com/lungcancer-anatomytopathologicalclassification-160709114825/85/Lung-cancer-anatomy-to-pathological-classification-23-320.jpg)
![• The base[basis pulmonis]- is broad, concave & rest on the convex surface of
diaphragm.
• Borders-
1. Inferior border- separates the base from the costal surface .
2. Posterior border- is broad & rounded& is received into the deep concavity on
either side of the vertebral column.
3. Anterior border- thin& sharp, and overlaps the front of pericardium.](https://image.slidesharecdn.com/lungcancer-anatomytopathologicalclassification-160709114825/85/Lung-cancer-anatomy-to-pathological-classification-24-320.jpg)


























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

