Downloaded 14 times


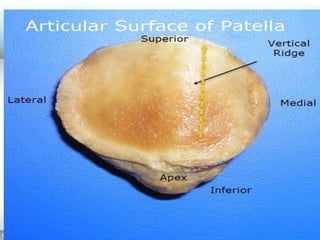












The patella is a triangular sesamoid bone located in the quadriceps tendon in front of the knee joint. It has three borders and two surfaces. The posterior surface articulates with the femur and is divided into medial and lateral facets. The patella attaches proximally to the quadriceps tendon and distally to the patellar ligament. During knee movement, different facets of the patella articulate with the femur. Clinical issues involving the patella include lateral dislocation and patellofemoral syndrome which is pain from cartilage breakdown on the patellar surfaces.






















































































