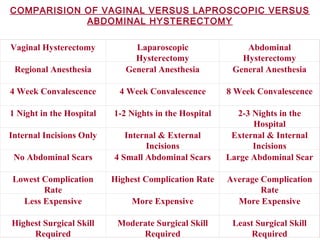
This document discusses laparoscopic assisted vaginal hysterectomy (LAVH). It begins with a brief history of laparoscopic hysterectomy and incidence rates of different hysterectomy methods from various studies. It then describes the classification, indications, procedure, complications, and comparison of LAVH, vaginal hysterectomy, and abdominal hysterectomy. While laparoscopic hysterectomy may be preferred for its minimal invasiveness, the document emphasizes that vaginal hysterectomy should be performed when possible to avoid unnecessary procedures. In conclusion, it states that the main goal of LAVH is to reduce abdominal hysterectomy rates by utilizing it where vaginal hysterectomy is contraindicated.


![“ DR. MANJUSHREE BOOB”
M.B.B.S. M.D. D.N.B. F.I.C.M.C.H.
DIPLOMATE OF NATIONAL BOARDS
FELLOW GUIDE FOR DAWN DGO’S COURSES
“SHUBHAM HOSPITAL”
BADNERA ROAD
AMRAVATI [ M.S. ]
By,…By,…](https://image.slidesharecdn.com/lavh1-170221121011/85/Lavh-1-2-320.jpg)
![INCIDENCE OF TAH, VH, LAVH
VALUE STUDY 1998 [ U. K. ]
[ Vaginal, Abdominal And Laparoscopic Uterine
Extirpation ]
Abdominal - 74%
Vaginal - 18.4%
Laparoscopic hysterectomy - 7.6% } 1995
U.S.A. STUDY BY KOVACK
Vaginal - 89%
Abdominal - 11%](https://image.slidesharecdn.com/lavh1-170221121011/85/Lavh-1-4-320.jpg)
![[ True state of the art Indian
Legacy]
[ Modern Surgery ]
Vaginal
Hysterectomy
L.A.V.H.](https://image.slidesharecdn.com/lavh1-170221121011/85/Lavh-1-7-320.jpg)
![TLH
[ Ultra Modern Surgery ]
Abdominal Hystectomy
[ AN OLD ART- NEED TO DECREASE THIS MORBID
SURGERY ]](https://image.slidesharecdn.com/lavh1-170221121011/85/Lavh-1-8-320.jpg)
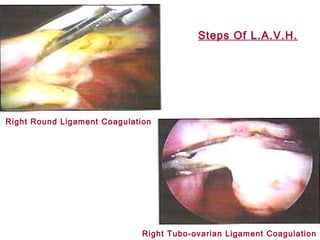

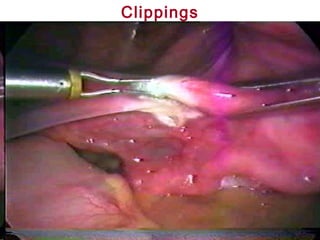


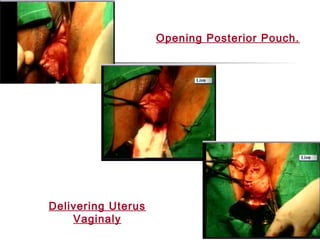
![-Surgical procedure involving dissection of tubovarian pedicle and
bladder dissection is done through Laparoscope - while vaginally
uterines are ligated under vision by delevering uterus through
colpotomy incision.
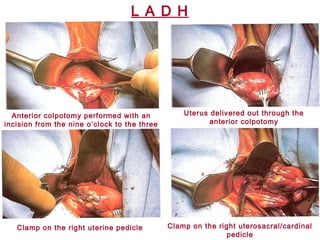
[ L A D H ]
Laparoscopic assisted Doderlein’s
Hysterectomy
Cutting the right infundibulopelvic
ligament
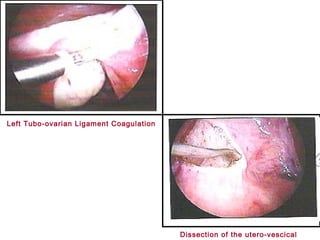
Dividing the peritoneum in the
uterovesicular pouch](https://image.slidesharecdn.com/lavh1-170221121011/85/Lavh-1-23-320.jpg)






































![[Challenge:Future] The Light Houseg](https://cdn.slidesharecdn.com/ss_thumbnails/challengefuture-the-light-houseg69-111206070710-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


