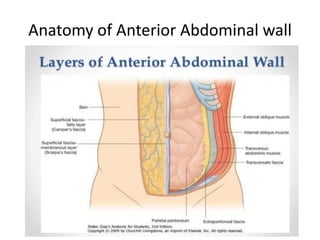
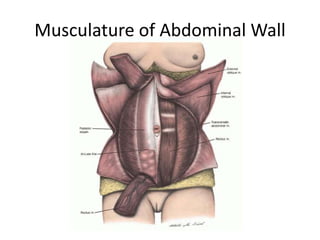
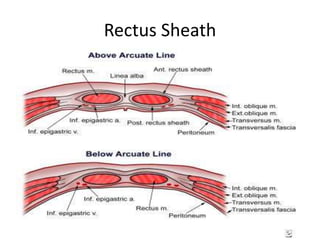
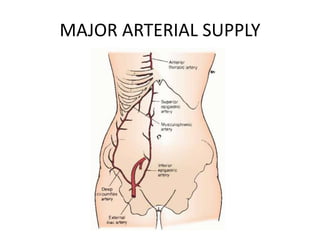
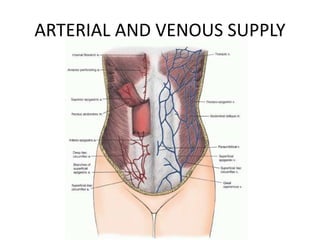
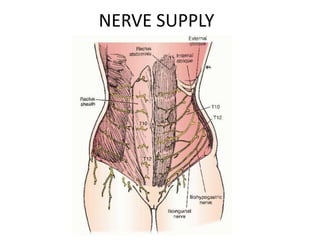
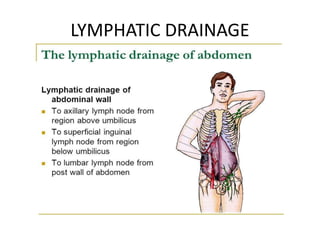
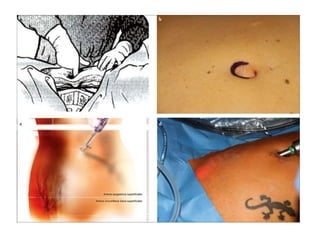
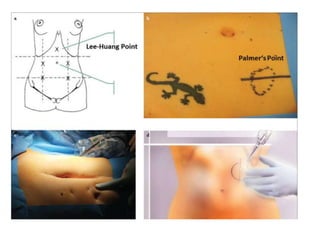
This document discusses the anatomy of the anterior abdominal wall and various incision types used for gynecological surgeries and laparotomies. It outlines the boundaries and musculature of the abdominal wall, including the rectus sheath. It then describes the advantages and disadvantages of transverse (including Pfannenstiel, Kustner, Cherney, and Maylard), vertical (including midline and paramedian), and oblique (including gridiron and Rockey-Davis) incisions. It also briefly mentions incisions used for cesarean sections and laparotomy port sites. The document provides detailed information on incision placement and exposure for different gynecological procedures.


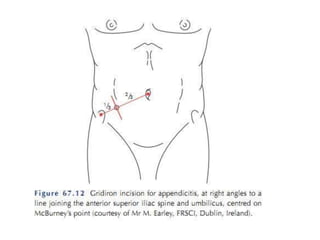
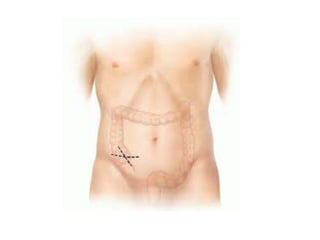








































![obg ppt [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obgpptautosaved-230216232416-2c9eedbf-thumbnail.jpg?width=640&height=640&fit=bounds)


















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








