Downloaded 28 times
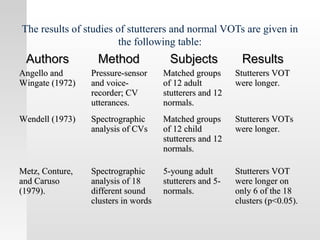
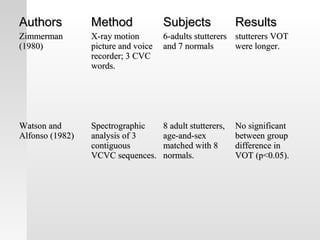
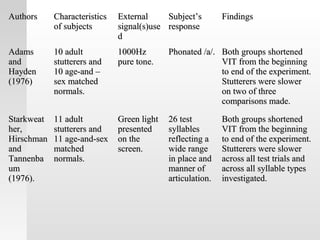
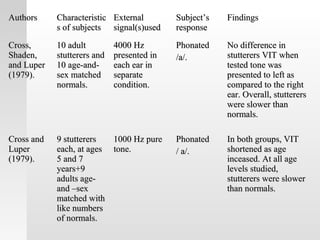
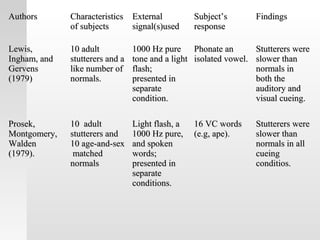
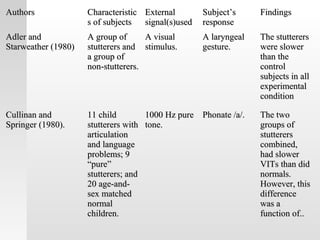
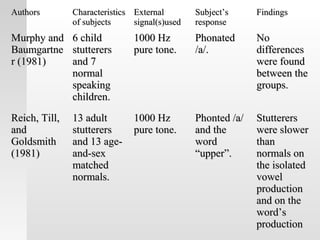
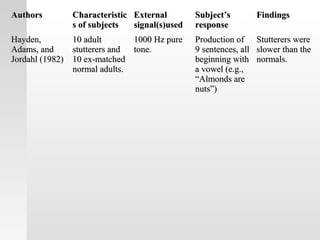


This document summarizes research on laryngeal dynamics in stuttering, specifically investigating voice onset time (VOT), voice initiation time (VIT), and speech initiation time (SIT) in stutterers versus normal speakers. Several studies are described that used instrumentation like spectrography, pressure sensors, and X-ray motion pictures to measure the time between articulatory gestures and voicing in stutterers and controls. Most findings showed stutterers had longer VOT, VIT and SIT than normal speakers, though some studies found no differences or differences only on some speech sounds. The research suggests laryngeal timing may be disrupted in stuttering.