Downloaded 35 times










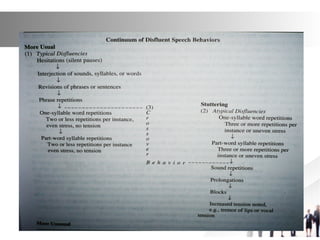





This document discusses fluency, factors that affect fluency, and dimensions of fluent speech. It defines fluency as effortless, continuous speech produced at a rapid rate. Factors that influence fluency include stress, sound duration, co-articulation, and effort. Disfluency refers to normal speech interruptions while dysfluency refers to stuttered interruptions. Dimensions of fluency include continuity, rate, duration, co-articulation, and effort. The document also discusses classifications of disfluencies and characteristics of stuttering as a disruption of fluent speech patterns.