Downloaded 369 times


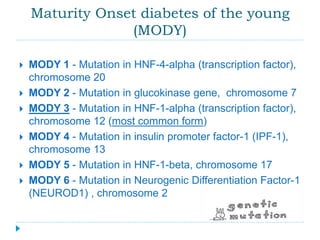
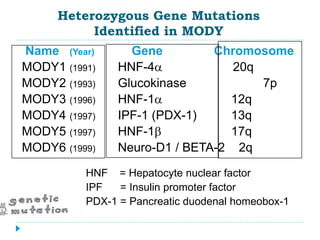

Latent autoimmune diabetes in adults (LADA) is often misdiagnosed as type 2 diabetes; it typically presents in individuals over 50 and progresses to insulin dependence within six years. Maturity-onset diabetes of the young (MODY) is characterized by genetic mutations affecting insulin secretion, resulting in early-onset type 2 diabetes and various treatment needs depending on the specific gene involved. Diagnosis for both conditions includes assessing symptoms, antibody testing, and C-peptide levels to differentiate from other diabetes types.











































![DM lecture for c1 [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/dmlectureforc1autosaved-220720190831-86418752-thumbnail.jpg?width=640&height=640&fit=bounds)