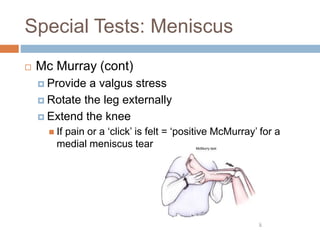
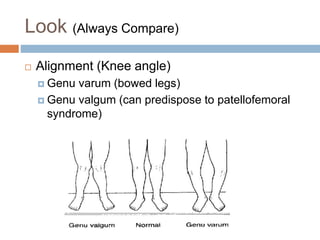
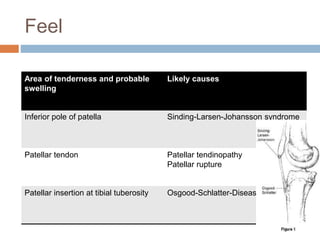
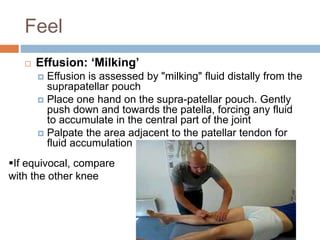
This document provides guidance on performing a thorough knee examination. It outlines steps to look, feel, move, and perform special tests on the knee to identify various injuries and conditions. The look section describes examining alignment, swelling, and other visual indicators. The feel section details palpating areas like the joint line, patella, and ligaments. Special tests are described to check the meniscus, collateral ligaments, cruciate ligaments, and other structures. It emphasizes comparing both knees and considering referrals from other joints.














![Special Tests: ACL
Sensitivity Specificity
Lachman test 85%[1] 94%[1]
Anterior Drawer test 68%[2] 79%[2]
Pivot Shift test 24%[1] 98%[1]
[1] Benjaminse A, Gokeler A, van der Schans CP. Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis.
J Orthop Sports Phys Ther. 2006 May;36(5):267-88.
[2] Kim SJ, Kim HK. Reliability of the anterior drawer test, the pivot shift test, and the Lachman test. Clin Orthop Relat Res. 1995 Aug;(317):2](https://image.slidesharecdn.com/kneeexamination-221115105810-179a5094/85/Knee-Examination-pptx-27-320.jpg)