Downloaded 33 times

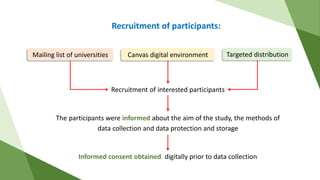
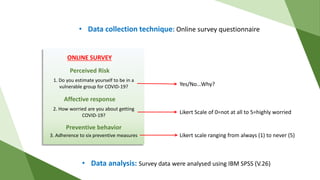
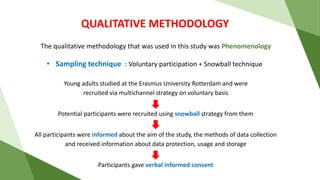
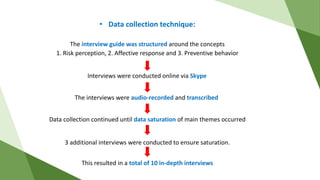
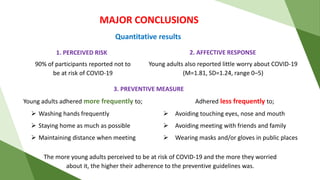
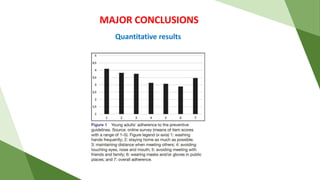
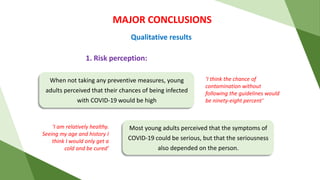




The document discusses a study examining the role of risk perception and affective response in COVID-19 preventive behaviors among young adults in the Netherlands, published in the BMJ Open journal. The study utilized a mixed methods approach, incorporating both quantitative surveys and qualitative interviews, to analyze the relationship between perceived risk, emotional responses, and adherence to preventive measures. Major findings indicate that higher risk perception and worry among participants correlated with increased adherence to COVID-19 guidelines, though overall adherence varied significantly among different behaviors.





































![[Bean survey] How Vietnamese people respond to COVID-19 outbreak in Vietnam](https://cdn.slidesharecdn.com/ss_thumbnails/beansurvey-coronavirus-v0-200318074802-thumbnail.jpg?width=640&height=640&fit=bounds)










![Epidemiology of Obesity [Global and Indian Scenario]]](https://cdn.slidesharecdn.com/ss_thumbnails/epidemiologyofobesity-241217054751-c5a2ec52-thumbnail.jpg?width=640&height=640&fit=bounds)






























