Downloaded 91 times


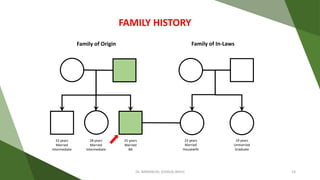



A 25-year-old male presents with symptoms of moderate depression, including decreased sleep, appetite, sadness, loss of interest, and guilt ideas, which have persisted for 3-4 months following marital stressors. His family history includes a father with a depressive disorder, and he was treated with escitalopram and clonazepam, showing adequate compliance. Non-pharmacological management recommendations include psychoeducation, addressing psychosocial stressors, and structured physical activity.















































![Epidemiology of Obesity [Global and Indian Scenario]]](https://cdn.slidesharecdn.com/ss_thumbnails/epidemiologyofobesity-241217054751-c5a2ec52-thumbnail.jpg?width=640&height=640&fit=bounds)































