OBJECTIVES
• Definition.
• Classificationand examples
• Types of synovial joints
• Joint stability
• Blood and nerve supply
• Movements at a joint
• Clinical correlations
3.
Introduction
• Also calledan articulation, derived from the
greek word athron.
• Definition: is a union or junction between two
or more bones or rigid parts of the skeleton.
• Function: movement, protection, weight
bearing/shock absorption.
4.
Classification of joints
Jointsare classified according to structure and function-
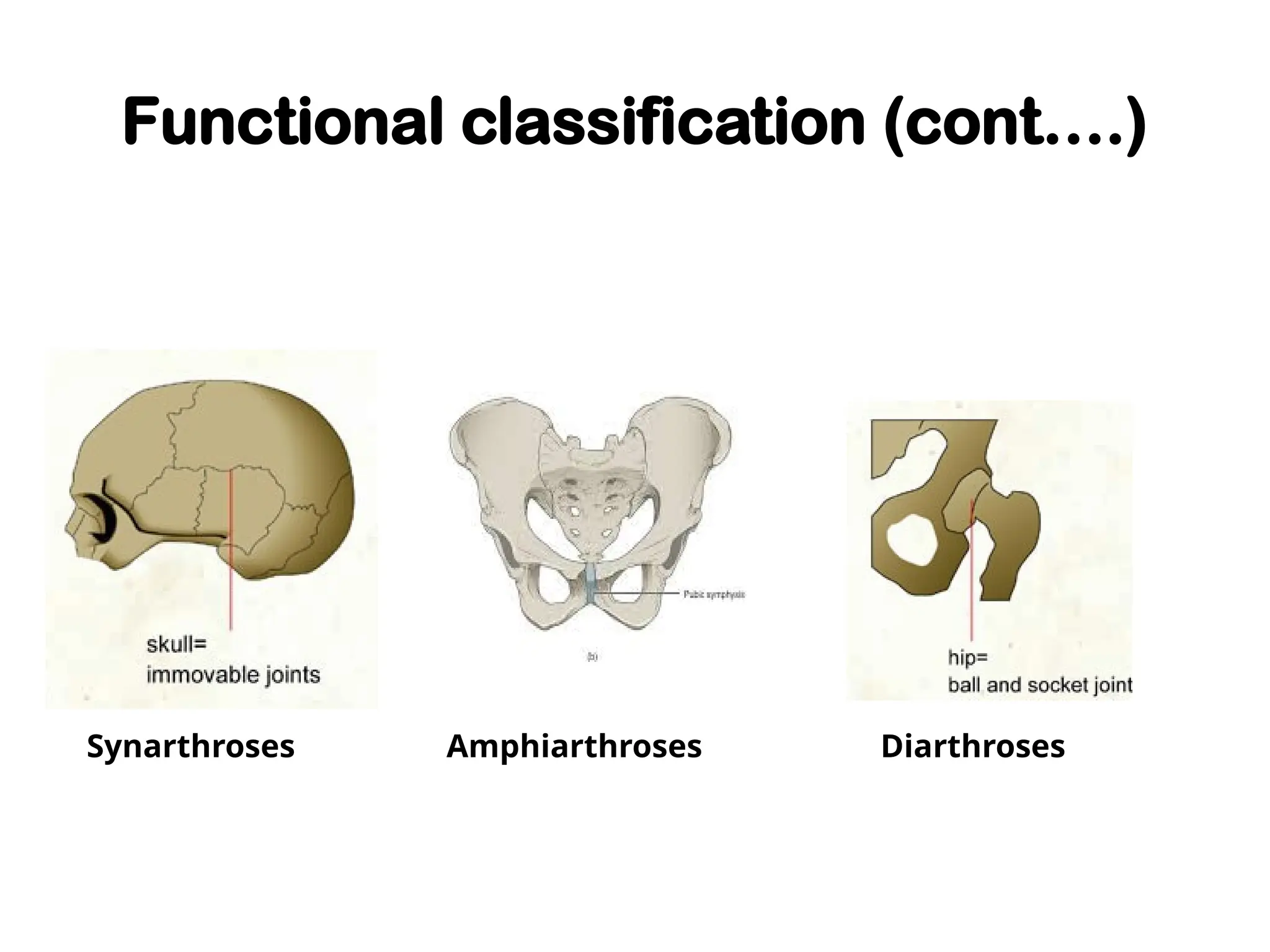
(A) Functional (based on degree of mobility):
1.Synarthroses: immovable joints (cranial sutures in
adults, primary cartilaginous joints in
growing children).
2.Amphiarthroses: slightly movable joints (joints
between adjacent laminae of vertebrae).
3.Diarthroses: freely movable joints (synovial joints).
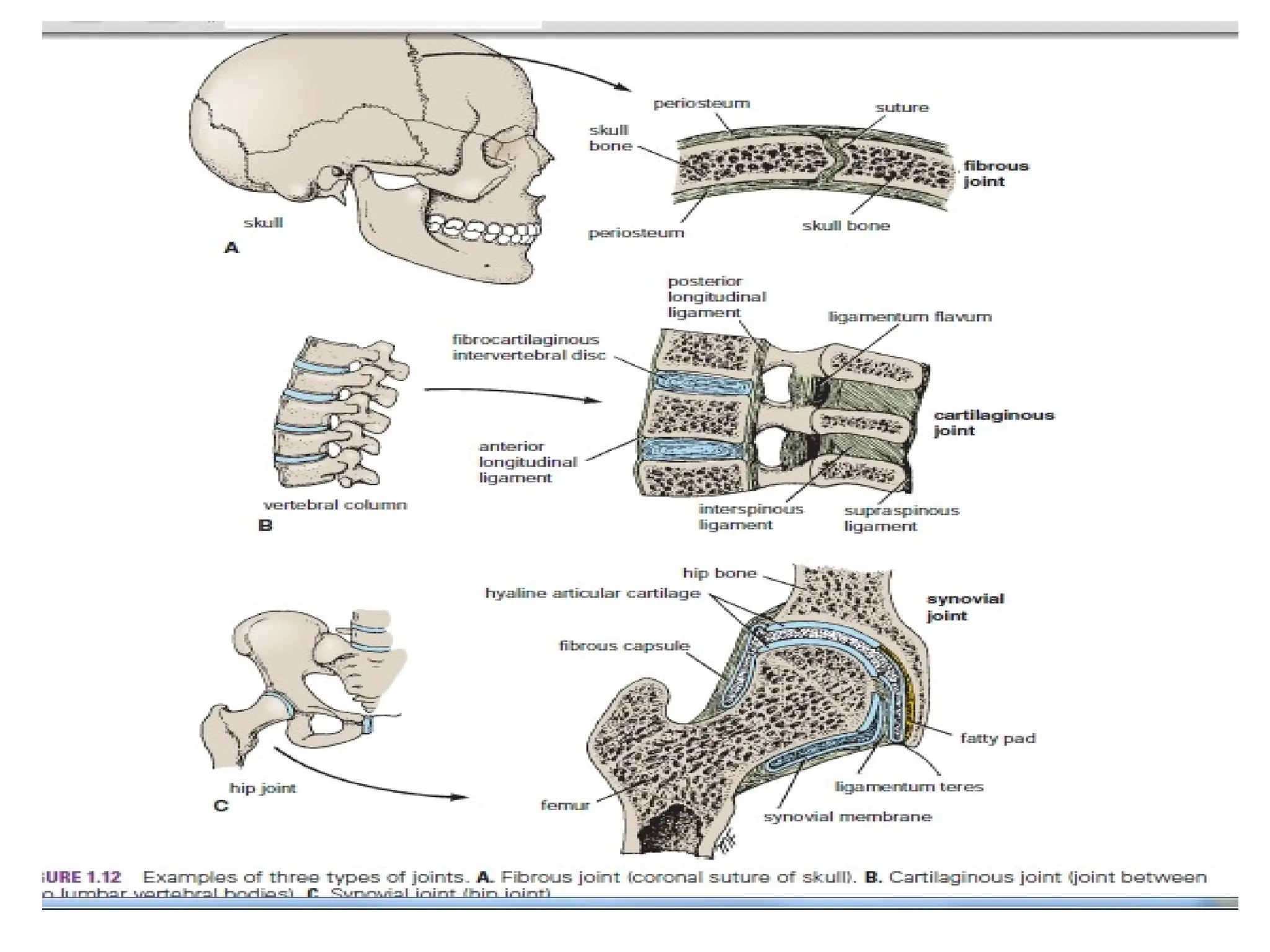
(B) Structural classification
Basedon type of connecting tissue and presence or
absence of joint cavity:
1. Fibrous: composed of intervening fibrous tissue with
no joint cavity. Immovable or slightly movable.
2. Cartilaginous: articulating bones are united by
cartilage (hyaline or fibrocartilage) with no joint cavity.
3. Synovial: articulating bones are separated by a fluid-
filled joint cavity.
8.
Fibrous joints
• Bonesare united by fibrous tissue.
• Range of movement depends on length of
fibres.
• May be a suture, syndesmosis, or gomphosis.
9.
Fibrous joints
1. Sutures:articular surfaces are connected by a thin layer of
connective tissue. They are confined to the skull and
are immovable.
2. Syndesmoses: bones are connected by a considerably greater
amount of connective tissue than in sutures in
the form of interosseous ligaments and
membranes. Slight movement is permitted.
e.g. interosseous tibiofibular joints,
interroseous radioulnar joints.
3. Gomphoses (peg and socket joint): articulation of teeth in
alveolar sockets of mandible and maxilla by
periodontal ligament.
• Serrate sutures-are most common interlocking
articulations, e.g. sagittal suture
• Squamous suture- bone overlaps bone, e.g between
temporal and parietal bones.
• Plane sutures- have edges which are fairly smooth e.g
maxillary suture between 2 halves of the hard palate.
• Synostosis- only found during skull growth between
halves of frontal bone, temporaly. If fusion does not
occur, its called a mytopic suture.
• Denticulate is tooth- like and found at lambdoid
suture.
• Schindylesis- wedge and groove joint, bones are joined
by fitting the ridge of one bone into the groove of
another.e.g between vomer and ethmoid bone.
13.
Cartilaginous joints
• Thearticulating structures of cartilaginous
joints are united by hyaline cartilage or
fibrocartilage.
• Grouped as primary cartilaginous joints/
synchondroses or secondary cartilaginous
joints.
14.
Primary cartilaginous joints
•Are Synchondroses
• the bones are united by
hyaline cartilage.
• permits slight bending
during early life.
• Usually temporary
unions. e.g epiphyseal
plates.
• permit growth in the
length of a bone.
15.
Secondary cartilaginous joints
•Also called symphyses.
• strong, slightly movable
joints united by
fibrocartilage.
• E.g. The fibrocartilaginous
intervertebral discs.
• provide strength and shock
absorption as well as
considerable flexibility to
the vertebral column
(spine).
16.
Synovial joints
• themost common type of joint
• Provide free movement between the bones they
join.
• are joints of locomotion, typical of nearly all
limb joints.
• usually reinforced by accessory ligaments that
are either separate (extrinsic) or are a thickening
of a portion of the joint capsule (intrinsic).
• Have a joint cavity filled with synovial fluid
• Often termed as diarthroses.
• articulating bonesunited by a joint (articular)
capsule (composed of an outer fibrous layer
lined by a serous synovial membrane)
spanning and enclosing an articular cavity.
• The joint cavity is a potential space that
contains a small amount of lubricating synovial
fluid, secreted by the synovial membrane.
• Inside the capsule, articular cartilage covers
the articulating surfaces of the bones; all other
internal surfaces are covered by synovial
membrane.
19.
Types of synovialjoints
The six major types of synovial joints are
classified according to;
• the shape of the articulating surfaces.
• the type/ plane of movement they permit.
• The number of articulating bones.
20.
Classification of Synovialjoints
(A) According to shape of articular surfaces:
1. Plane
2. Hinge
3. Pivot
4. Condylar
5. Ellipsoid
6. Saddle
7. Ball and socket
21.
Plane joints
• permitgliding or sliding
movements in the plane of
the articular surfaces. The
opposed surfaces of the
bones are flat or almost
flat, with movement
limited by their tight joint
capsules. Examples are the
acromioclavicular joint,
intercarpal and intertarsal
joints.
Saddle joints
• permitabduction and
adduction as well as flexion
and extension, movements
occurring around two axes
at right angles to each
other; thus saddle joints are
biaxial joints that allow
movement in two planes,
sagittal and frontal.
Examples- the
carpometacarpal joint at
the base of the 1st digit
(thumb), sterno-clavicular .
24.
Hinge joints
• Articularsurfaces are pulley
shaped.
• permit flexion and extension only,
movements that occur in one
plane (sagittal) around a single
axis that runs transversely; thus
hinge joints are uniaxial joints.
• The joint capsule of these joints is
thin and lax anteriorly and
posteriorly where movement
occurs; however, the bones are
joined by strong, laterally placed
collateral ligaments. e.g. elbow,
knee, ankle and interphalangeal
joints.
25.
Ellipsoid joint
• anelliptical convex
articular surface fits into
an elliptical concave
articular surface. The
movements of flexion,
extension, abduction,and
adduction can take place,
but rotation is impossible.
• The wrist, and atlanto-
occipital joints are good
examples.
26.
Ball and asocket
•Allow movement in multiple
axes and planes: flexion and
extension, abduction and
adduction,medial and lateral
rotation, and circumduction;
thus ball and socket joints
are multiaxial joints.
• In these highly mobile joints,
the spheroidal surface of
one bone moves within the
socket of another. E.g. hip,
shoulder joints.
27.
condyloid
• Round articularsurface of one
bone fits into a socket-type
articular surface of another
bone.
• permit flexion and extension as
well as abduction and
adduction; thus condyloid joints
are also biaxial. However,
movement in one plane
(sagittal) is usually greater
(freer) than in the other..
E.g.The metacarpophalangeal
joints (knuckle joints), temporo-
mandibular
28.
Pivot joints (Trochoidjoints)
• permit rotation around a central
axis; thus they are uniaxial.
• In these joints, a rounded process
of bone rotates within a sleeve or
ring. The median atlantoaxial joint
is a pivot joint.
• Rounded end of one bone fits into
the concavity of
another bone.
• The rounded part
is surrounded by a ligament.
• Limited rotation
around a central axis.
• e.g. superior radio-ulnar and
median atlanto-axial joints.
29.
(B) According toplane of movements
• Uniaxial: Hinge and Pivot
• Biaxial: Condylar, ellipsoid, saddle
• Multiaxial: Ball and socket
Uniaxial Biaxial Multiaxial
30.
(C) According tonumber of articulating bones
• Simple (2 bones)
• Compound (more than 2 bones)
31.
Joint stability
The stabilityof a joint depends on three main factors:
1)the shape, size, and arrangement (relative proportion of
the articular surfaces
2)the ligaments;
3)the tone of the muscles around the joint. The more stable a
joint is, the less the range of movement at the joint.
32.
Blood supply
• Jointsreceive blood from articular arteries
that arise from the vessels around the joint.
The arteries often anastomose (communicate)
to form networks (peri-articular arterial
anastomoses) to ensure a blood supply to and
across the joint in the various positions
assumed by the joint.
33.
Nerve supply toa joint
• Joints have a rich nerve supply provided by
articular nerves with sensory nerve endings in
the joint capsule. In the distal parts of the
limbs (hands and feet), the articular nerves
are branches of the cutaneous nerves
supplying the overlying skin. However, most
articular nerves are branches of nerves that
supply the muscles that cross and therefore
move the joint.
34.
• The Hiltonlaw states that the nerves supplying a
joint also supply the muscles moving the joint and
the skin covering their distal attachments. Articular
nerves transmit sensory impulses from the joint
that contribute to the sense of proprioception,
which provides an awareness of movement and
position of the parts of the body.
• The synovial membrane is relatively insensitive.
• Pain fibers are numerous in the fibrous layer of the
joint capsule and the accessory ligaments, causing
considerable pain when the joint is injured. The
sensory nerve endings respond to the twisting and
stretching that occurs during sports activities.
Special movements:
1. Inversion:movement of the foot medially
2. Eversion: movement of the foot laterally
3. Protraction: movement of the mandible forward
4. Retraction: movement of the protracted part back
to its starting position
5. Elevation: lifting a body part superiorly
6. Depression: moving the elevated part inferiorly
7. Opposition: touching the thumb to the tips of
other fingers
8. Plantar flexion
9. Dorsiflexion
37.
Clinical correlations/Further reading
•Arthritis- inflammation of a joint
• Dislocation and subluxation- abnormal
separation of bones in a joint. Sublaxation is
partial.
• Sprains- tearing of ligaments connecting bones
and joints
• Bursitis- inflammation of fluid filled pads/
bursae that act as a cussion at a joint.
• Protheses and Bionics- biologically inspired
engineering to replace organs by mechanical
versions.
38.
To read
• Fontanellesand their role in child birth
• Aging effects on joints
• arthroscopy













































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)










